




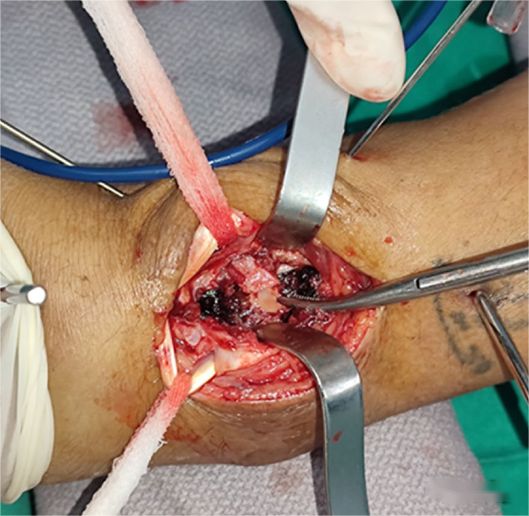
The most common treatment for distal radius fractures is the volar Henry approach with the use of locking plates and screws for internal fixation. During the internal fixation procedure, it is typically not necessary to open the radiocarpal joint capsule. Joint reduction is achieved through an external manipulation method, and intraoperative fluoroscopy is used to assess joint surface alignment. In cases of intra-articular depressed fractures, such as Die-punch fractures, where indirect reduction and assessment are challenging, it may be necessary to use a dorsal approach to assist with direct visualization and reduction (as shown in the figure below).
The extrinsic ligaments and intrinsic ligaments of the radiocarpal joint are considered important structures for maintaining wrist joint stability. With advances in anatomical research, it has been discovered that, under the condition of preserving the integrity of the short radiolunate ligament, cutting the extrinsic ligaments does not necessarily result in wrist joint instability.

Therefore, in certain situations, to achieve a better view of the joint surface, it may be necessary to partially incise the extrinsic ligaments, and this is known as the volar intraarticular extended window approach (VIEW). As shown in the figure below:
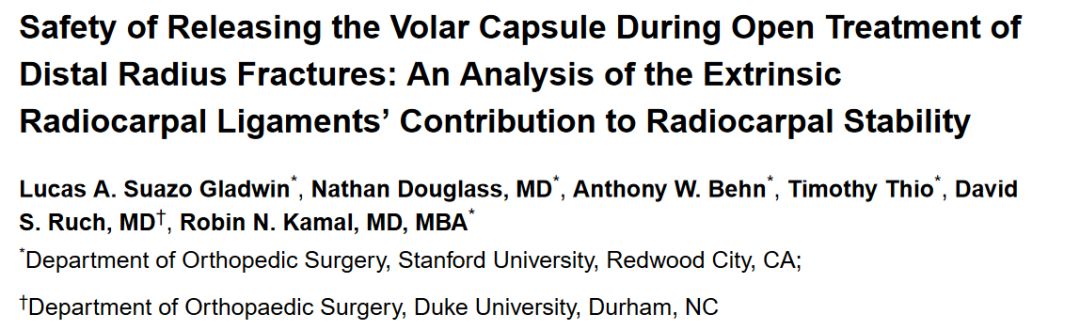
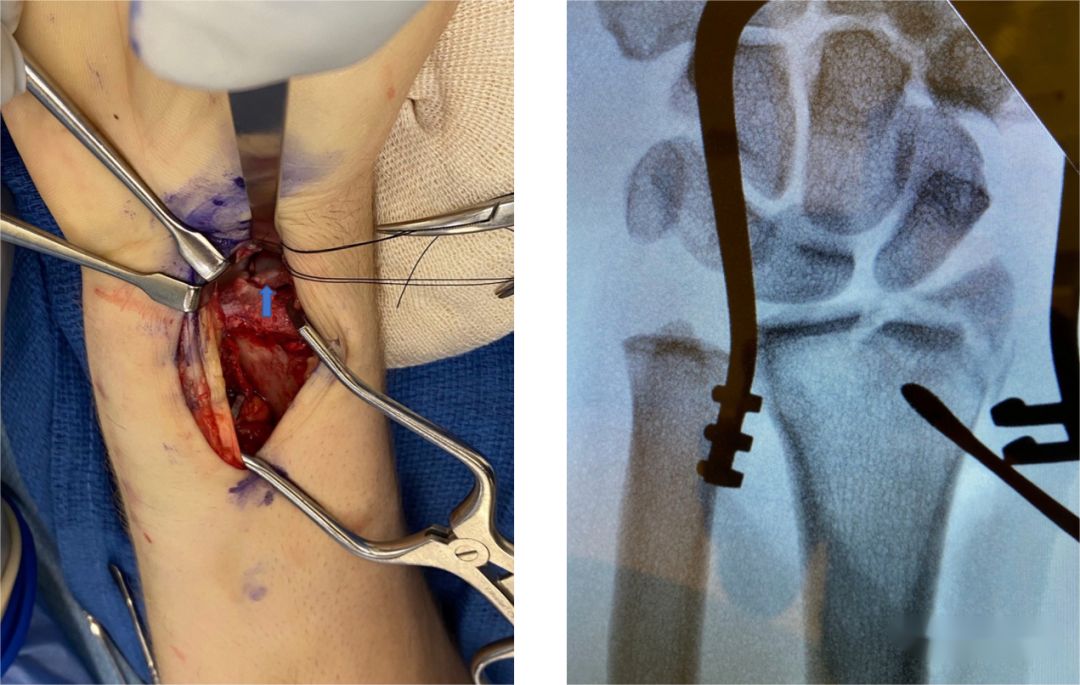
Figure A-B: In the conventional Henry approach for exposing the distal radius bone surface, in order to access a split fracture of the distal radius and scaphoid facet, the wrist joint capsule is initially incised. A retractor is used to protect the short radiolunate ligament. Subsequently, the long radiolunate ligament is incised from the distal radius towards the ulnar side of the scaphoid. At this point, direct visualization of the joint surface can be achieved.
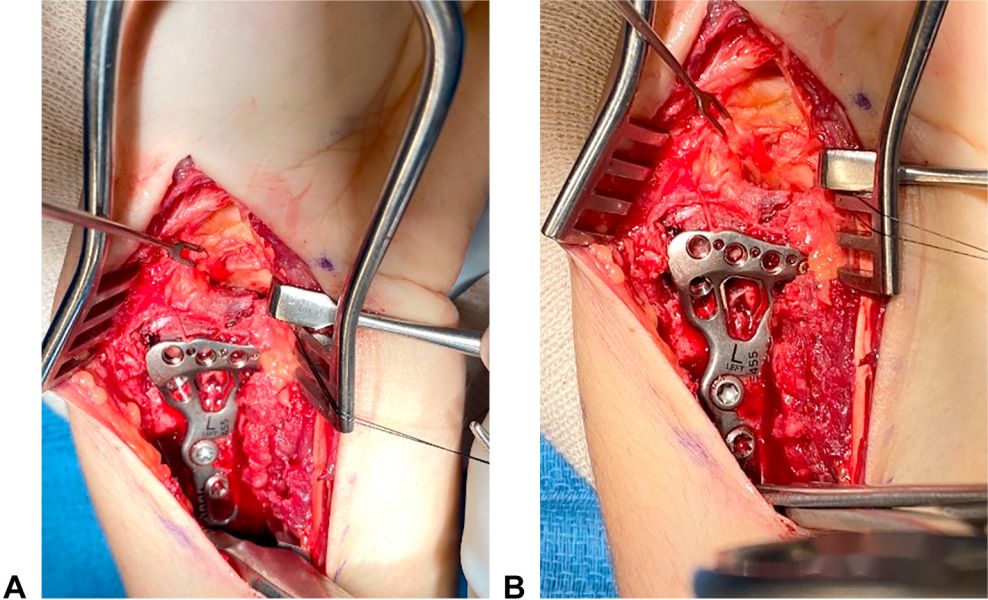
Figure C-D: After exposing the joint surface, reduction of the sagittal plane depressed joint surface is performed under direct visualization. Bone elevators are used to manipulate and reduce the bone fragments, and 0.9mm Kirschner wires may be used for temporary or final fixation. Once the joint surface is adequately reduced, standard methods for plate and screw fixation are followed. Finally, the incisions made in the long radiolunate ligament and the wrist joint capsule are sutured.
The theoretical basis of the VIEW (volar intraarticular extended window) approach lies in the understanding that cutting certain wrist joint extrinsic ligaments does not necessarily result in wrist joint instability. Therefore, it is recommended for certain complex intra-articular comminuted distal radius fractures where fluoroscopic joint surface reduction is challenging or when step-offs are present. The VIEW approach is strongly recommended to achieve a better direct visualization during reduction in such cases.
Post time: Sep-09-2023





