




Femoral neck fracture is a relatively common and potentially devastating injury for orthopaedic surgeons, with a high incidence of non-union and osteonecrosis due to the fragile blood supply. Accurate and good reduction of femoral neck fractures is the key to successful internal fixation.
Evaluation of Reduction
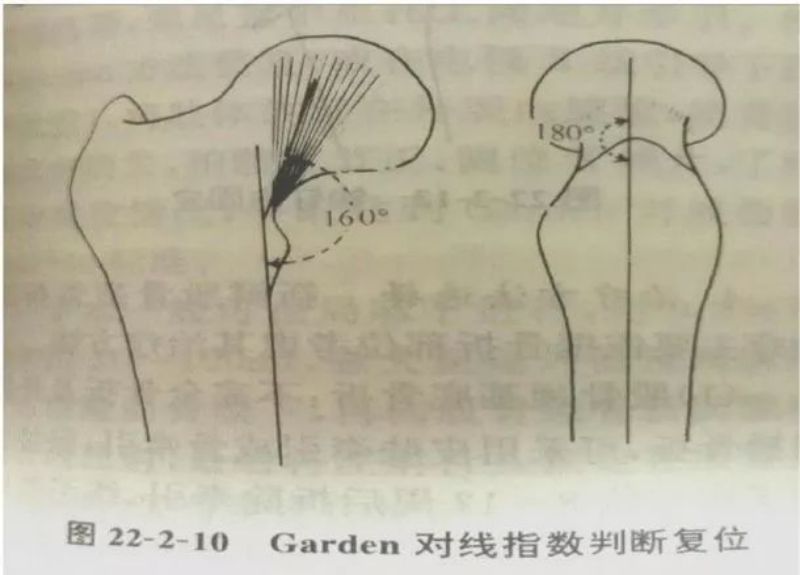
According to Garden, the standard for reduction of displaced femoral neck fracture is 160° in the orthopedic film and 180° in the lateral film. It is considered acceptable if the Garden index is between 155° and 180° in the medial and lateral positions after reduction.
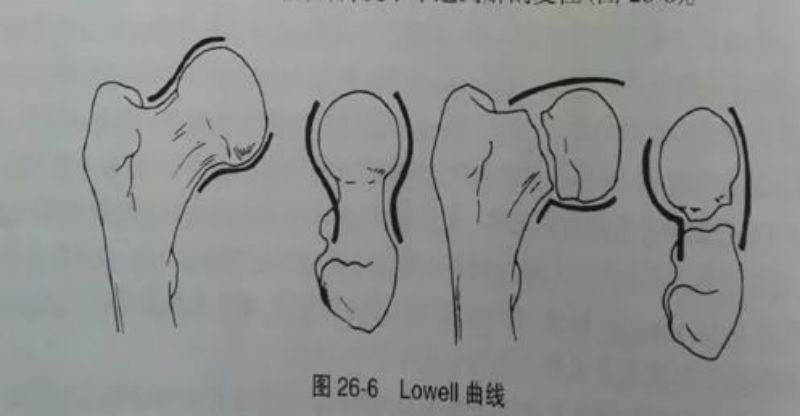
X-ray evaluation: after closed reduction, the degree of satisfaction of reduction should be determined by using high-quality X-ray images.Simom and Wyman have performed different angles of X-ray after closed reduction of femoral neck fracture, and found that only the positive and lateral X-ray films show anatomical reduction, but not the real anatomical reduction.Lowell suggested that the convex surface of the femoral head and the concave surface of the femoral neck can be connected to an S-curve in the normal anatomical situation. Lowell suggested that the convex surface of the femoral head and the concave surface of the femoral neck can form an S-shaped curve under normal anatomical conditions, and once the S-shaped curve is not smooth or even tangent in any position on the X-ray, it suggests that anatomical repositioning has not been achieved.
Inverted triangle has more obvious biomechanical advantages
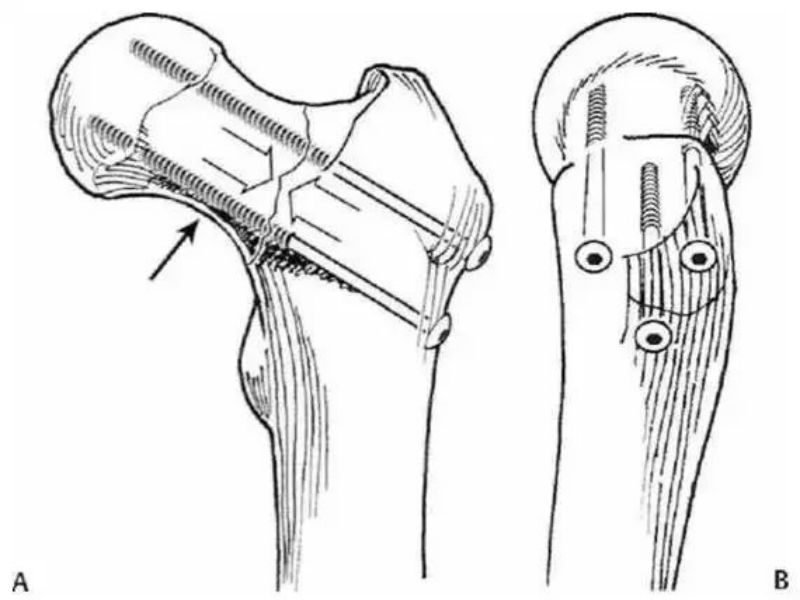
As an example, in the figure below, after a fracture of the neck of the femur, the fracture end is subjected to stresses that are predominantly tensile in the upper part and compressive in the lower part.
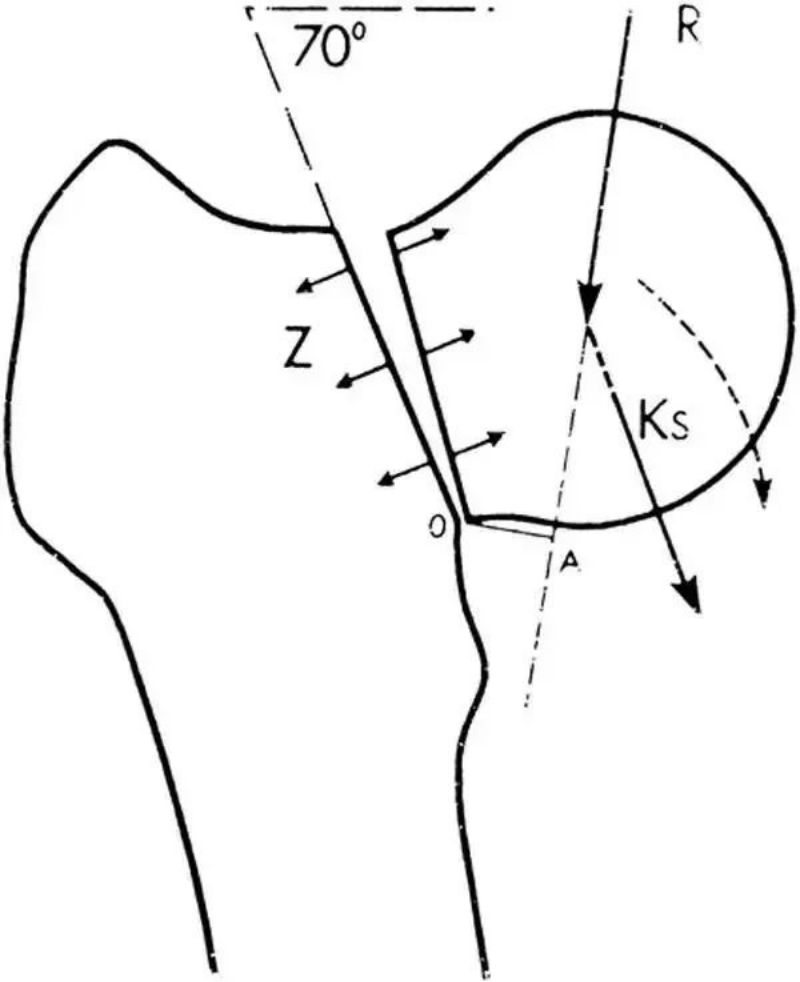
The objectives of fracture fixation are:1. to maintain good alignment and 2. to counteract tensile stresses as much as possible, or to convert tensile stresses into compressive stresses, which is consistent with the principle of tension banding. Therefore, the inverted triangle solution with 2 screws above is clearly superior to the orthotic triangle solution with only one screw above to counteract tensile stress.
The order in which the 3 screws are placed in a femoral neck fracture is important:
The first screw should be the tip of the inverted triangle, along the femoral moment;
The second screw should be placed posterior to the base of the inverted triangle, along the femoral neck;
The third screw should be anterior to the bottom edge of the inverted triangle, on the tension side of the fracture.
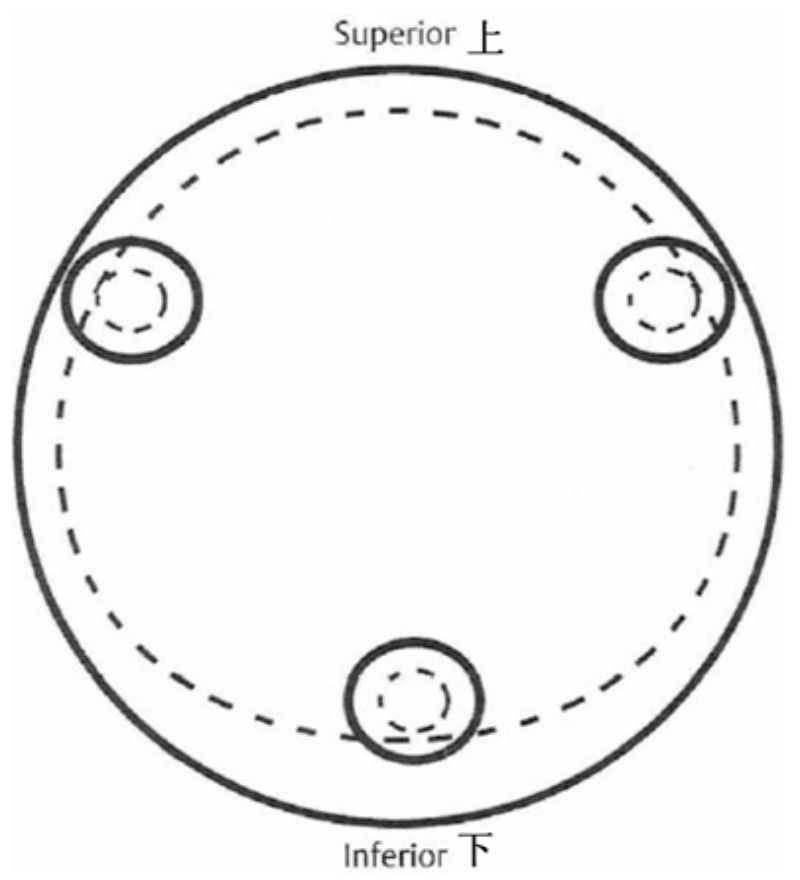
Since femoral neck fractures are most often associated with osteoporosis, screws have limited screw grip if they are not attached to the edge and bone mass is sparse in the middle position, so attaching the edge as close as possible to the subcortex provides better stability. Ideal position:
Three principles of fixing hollow nails: close to the edge, parallel, inverted products
Adjacent means that the 3 screws are within the neck of the femur, as close to the peripheral cortex as possible. In this way, the 3 screws as a whole create a surface pressure on the entire fracture surface, whereas if the 3 screws are not sufficiently discrete, the pressure tends to be more point-like, less stable and less resistant to torsion and shear.
Postoperative Functional Exercises
Toe-pointing weight-bearing exercises can be performed for 12 weeks after fracture fixation, and partial weight-bearing exercises can be started after 12 weeks. In contrast, for Pauwels type III fractures, fixation with DHS or PFNA is recommended.
Post time: Jan-26-2024





