




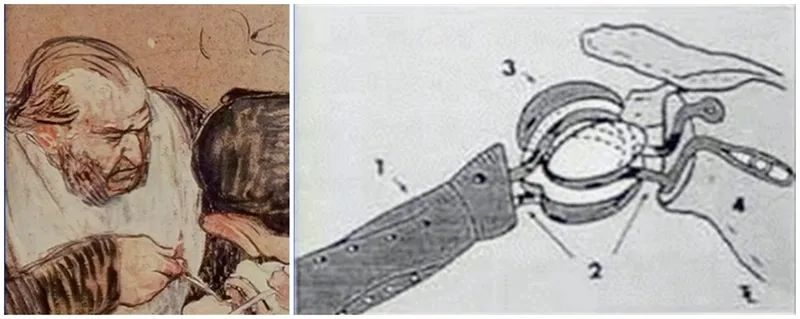
The concept of artificial shoulder replacement was first proposed by Themistocles Gluck in 1891. The artificial joints mentioned and designed together include hip, wrist, etc. The first shoulder replacement surgery was performed on a patient in 1893 by French surgeon Jules Emile Péan at the Hôpital International in Paris on a 37-year-old patient with tuberculosis of the joints and bones The first documented shoulder arthroplasty. The prosthesis was made by dentist J. Porter Michaels from Paris, and the humeral stem was made of platinum metal and attached to a paraffin-coated rubber head by wire to form a constrained implant. The patient's initial results were satisfactory, but the prosthesis was eventually removed after 2 years due to multiple recurrences of tuberculosis. This is the first attempt made by humans in artificial shoulder replacement.
In 1951, Frederick Krueger reported the use of a more anatomically significant shoulder prosthesis made of vitamins and molded from the proximal humerus of a cadaver. This was successfully used to treat a young patient with osteonecrosis of the humeral head
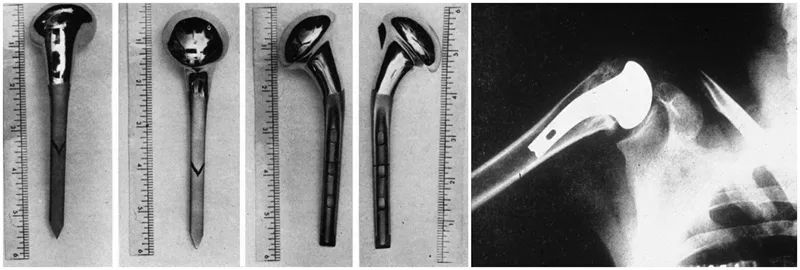
But the truly modern shoulder replacement was designed and developed by shoulder guru Charles Neer. In 1953, in order to solve the unsatisfactory results of its surgical treatment of proximal humeral fractures, Neer developed an anatomical proximal humeral prosthesis for humeral head fractures, which was improved several times in the following two decades, respectively. Designed second and third generation prostheses.
In the early 1970s, in order to solve the shoulder replacement in patients with severe rotator cuff dysfunction, the concept of reverse shoulder arthroplasty (RTSA) was first proposed by Neer, but due to the early failure of the glenoid component, The concept was subsequently abandoned. In 1985, Paul Grammont improved according to the concept proposed by Neer, moving the center of rotation medially and distally, changing the moment arm and tension of the deltoid, thus perfectly solving the problem of rotator cuff function loss.
Design principles of the trans-shoulder prosthesis
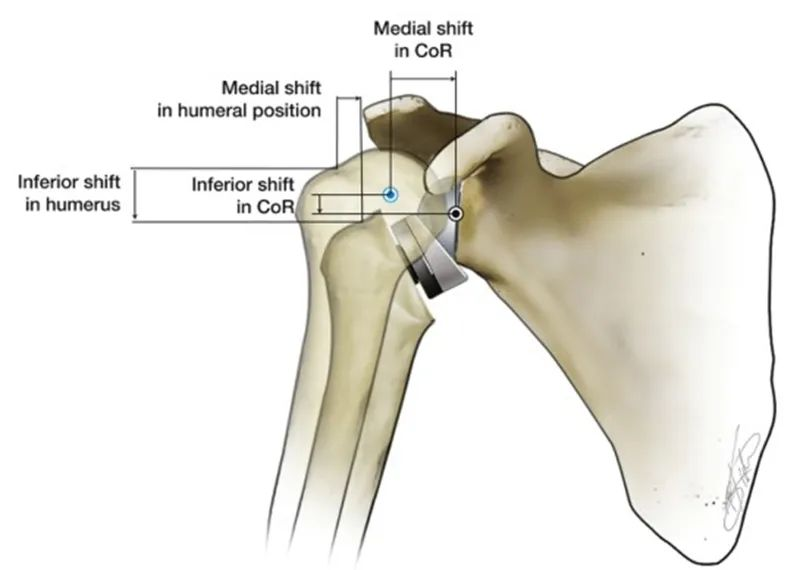
Reverse shoulder arthroplasty (RTSA) reverses the anatomical relationship of the natural shoulder to restore shoulder stability. RTSA creates a fulcrum and center of rotation (CoR) by making the glenoid side convex and the humeral head side concave. The biomechanical function of this fulcrum is to prevent the humeral head from moving upward when the deltoid muscle contracts to abduct the upper arm. The feature of RTSA is that the rotation center of the artificial shoulder joint and the position of the humeral head relative to the natural shoulder are moved inward and downward. Different RTSA prosthesis designs are different. The humeral head is moved down by 25~40mm and moved inward by 5~20mm.
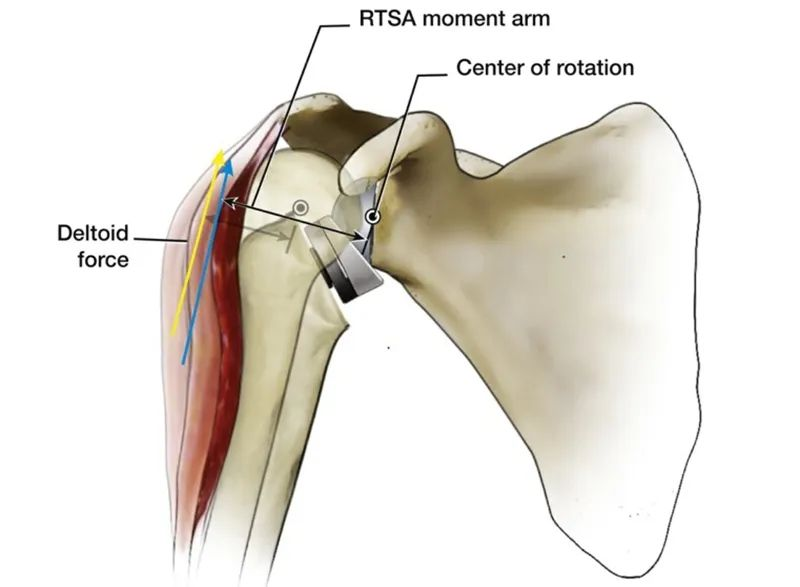
Compared with the natural shoulder joint of the human body, an obvious advantage of internal shifting CoR is that the abduction moment arm of the deltoid is increased from 10mm to 30mm, which improves the abduction efficiency of the deltoid, and less muscle force can be generated. The same torque, and this feature also makes the abduction of the humeral head no longer completely dependent on the depression function of the complete rotator cuff.
This is the design and biomechanics of RTSA, and it may be a little boring and difficult to understand. Is there a simpler way to understand it? The answer is yes.
The first is the design of the RTSA. Carefully observe the characteristics of each joint of the human body, we can find some rules. Human joints can be roughly divided into two categories. One is near-trunk joints like shoulders and hips, with the proximal end being the "cup" and the distal end being the "ball".
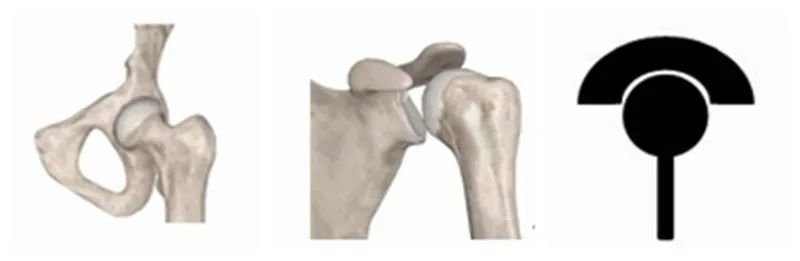
The other type is distal joints such as knees and elbows, with the proximal end being the "ball" and the distal end being the "cup".

The plan adopted by medical pioneers when designing artificial shoulder joint prostheses in the early days was to restore the anatomical structure of the natural shoulder as much as possible, so all plans were designed with the proximal end as a "cup" and the distal end as a "ball". Some researchers even deliberately designed the "cup" to be larger and deeper in order to increase the stability of the joint, similar to the human hip joint, but it was later proved that increasing the stability actually increased the failure rate, so this design was quickly adopted. give up. RTSA, on the other hand, reverses the anatomical characteristics of the natural shoulder, inverting the "ball" and "cup", making the original "hip" joint more like an "elbow" or "knee". This subversive change finally solved many difficulties and doubts of artificial shoulder replacement, and in many cases, its long-term and short-term efficacy has been significantly improved.
Likewise, the design of the RTSA shifts the center of rotation to allow for increased deltoid abduction efficiency, which may also sound obscure. And if we compare our shoulder joint to a seesaw, it's easy to understand. As shown in the figure below, applying the same torque in the A direction (the deltoid contraction force), if the fulcrum and starting position are changed, it is obvious that a larger torque (the upper arm abduction force) can be generated in the B direction.
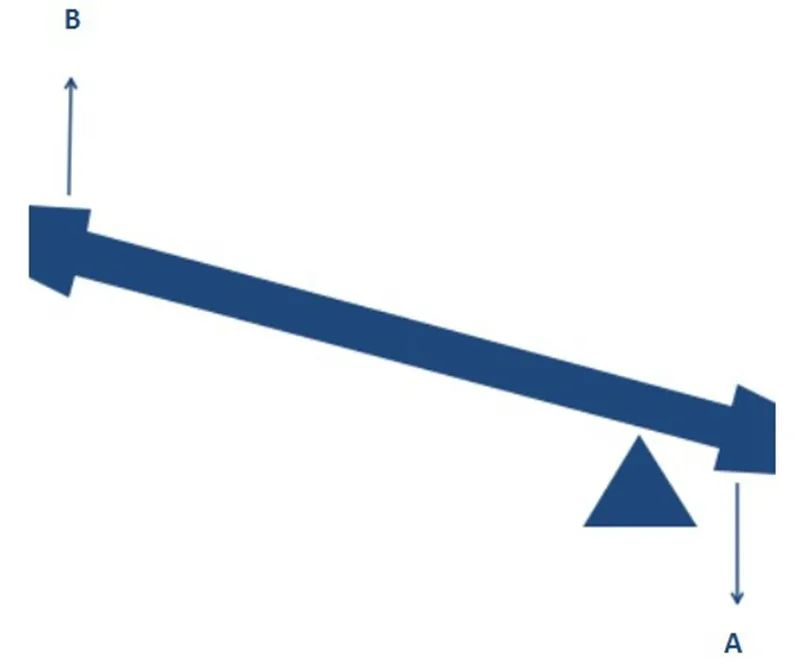
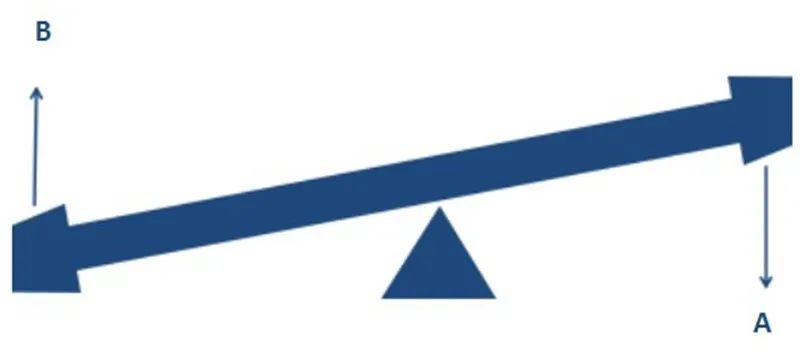
A change in the RTSA's center of rotation has a similar effect, allowing a destabilized shoulder to initiate abduction without the rotator cuff depression. As Archimedes said: Give me a fulcrum and I can move the whole earth!
RTSA Indications and Contraindications
The classic indication for RTSA is rotator cuff tear arthropathy (CTA), a giant rotator cuff tear with osteoarthritis, which is typically characterized by upward displacement of the humeral head, resulting in the glenoid , acromion and humeral head continued degenerative changes. The upward displacement of the humeral head is caused by an unbalanced force couple under the action of the deltoid after rotator cuff dysfunction. CTA is more common in older women, where a classic "pseudoparalysis" may occur.
The use of shoulder arthroplasty, especially RTSA, has increased substantially over the past two decades. Based on the initial successful results of RTSA application, the continuous development of surgical technique, and the proficient application of this technique, the initial narrower indications for RTSA have been expanded, and therefore, most shoulder arthroplasty procedures currently performed are RTSA.
For example, anatomical total shoulder arthroplasty (ATSA) was the preferred choice for shoulder osteoarthritis without rotator cuff tear in the past, but in recent years, the number of people who hold this view seems to be gradually decreasing. There are the following aspects. Reasons have led to this trend. First, up to 10% of patients who receive ATSA already have a rotator cuff tear. Second, in some cases, the "structural" integrity of the "function" of the rotator cuff is not complete, especially in some elderly patients. Finally, even if the rotator cuff is intact at the time of surgery, rotator cuff degeneration occurs with age, especially after ATSA procedures, and there is indeed a great deal of uncertainty about the function of the rotator cuff. This phenomenon usually occurs in elderly patients older than 70 years. Therefore, more and more surgeons began to choose RTSA when facing pure shoulder osteoarthritis. This situation has led to a new thinking that RTSA may also be the first choice for patients with osteoarthritis with an intact rotator cuff based solely on age.
Similarly, in the past, for irreparable massive rotator cuff tears (MRCT) without osteoarthritis, alternative methods include subacromial decompression, partial rotator cuff reconstruction, Chinese way, and upper joint capsule reconstruction. , the success rate varies. Based on the proficiency and successful application of RTSA in various situations, more and more operators have recently tried RTSA in the face of simple MRCT, and it has been very successful, with a 10-year implantation survival rate of over 90%.
In summary, in addition to CTA, the current expanded indications for RTSA include large irreparable rotator cuff tears without inflammatory osteoarthropathy, tumors, acute fractures, post-traumatic arthritis, bone defects or severely deformed bone joints. inflammation, and recurrent shoulder dislocations.
There are few contraindications to RTSA. Except for the general contraindications of artificial joint replacement such as infection, non-function of the deltoid muscle is an absolute contraindication to RTSA. In addition, for proximal humerus fractures, open fractures and brachial plexus injuries should also be considered contraindications, while isolated axillary nerve injuries should be considered relative contraindications.
Post-operative care and rehabilitation
Principles of postoperative rehabilitation:
Mobilize patients' enthusiasm for rehabilitation and establish reasonable expectations for patients.
Reduces pain and inflammation, and protects healing structures, but subscapularis usually does not need to be protected.
Anterior dislocation of the shoulder joint is likely to occur at the end positions of hyperextension, adduction and internal rotation, or abduction and external rotation. Therefore, movements such as backhands should be avoided for 4 to 6 weeks after the operation. These positions have the risk of dislocation.
After 4 to 6 weeks, it is still necessary to communicate with and obtain permission from the surgeon before starting the above movements and positions.
Postoperative rehabilitation exercises should be performed first without weight-bearing and then with weight-bearing, first without resistance and then with resistance, first passively and then actively.
At present, there is no strict and uniform rehabilitation standard, and there are great differences in different researchers' plans.
Patient activities of daily living (ADLs) strategy (0-6 weeks):

Dressing

Sleep
Daily exercise strategy (0-6 weeks):

Active elbow flexion

Passive shoulder flexion
Sichuan Chenanhui Techonology Co.,Ltd.
Whatsapp:+8618227212857
Post time: Nov-21-2022





