




Distal radius fracture is one of the most common joint injuries in clinical practice, which can be divided into mild and severe. For mildly non-displaced fractures, simple fixation and appropriate exercises can be used for recovery; however, for severely displaced fractures, manual reduction, splint or plaster fixation should be used; for fractures with obvious and severe damage to the articular surface, Surgical treatment is required.
PART 01
Why is the distal radius prone to fracture?
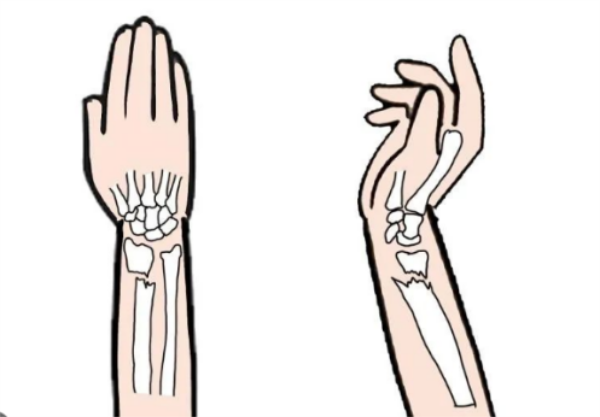
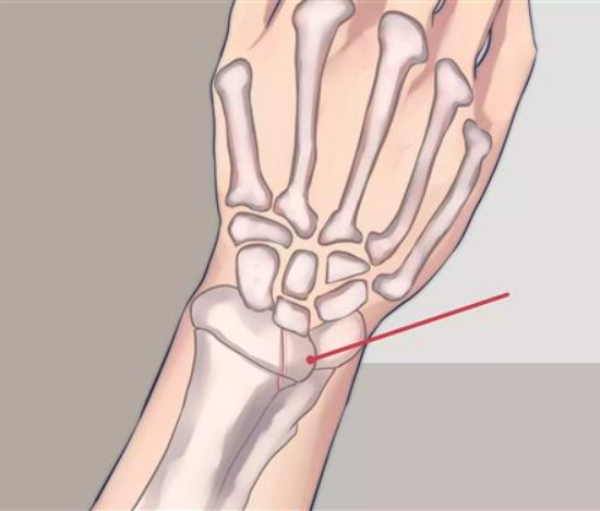
Since the distal end of the radius is the transition point between cancellous bone and compact bone, it is relatively weak. When the patient falls and touches the ground, and the force is transmitted to the upper arm, the distal end of the radius becomes the point where the stress is most concentrated, resulting in a fracture. This type of fracture occurs more frequently in children, because children's bones are relatively small and not strong enough.

When the wrist is injured in the extended position and the palm of the hand is injured and fractured, it is called an extended distal radius fracture (Colles), and more than 70% of them are of this type. When the wrist is injured in the flexed position and the back of the hand is injured, it is called a flexed distal radius fracture (Smith). Some typical wrist deformities are prone to occur after distal radius fractures, such as "silver fork" deformity, "gun bayonet" deformity, etc.
PART 02
How are distal radius fractures treated?
1. Manipulative reduction + plaster fixation + unique Honghui traditional Chinese medicine ointment application
For the vast majority of distal radius fractures, satisfactory results can be obtained through precise manual reduction + plaster fixation + traditional Chinese medicine application.
Orthopedic surgeons need to adopt different positions for fixation after reduction according to different types of fractures: Generally speaking, Colles (extension type distal radius fracture) fractures should be fixed at 5°-15° of palmar flexion and maximum ulnar deviation; Smith The fracture (flexion distal radius fracture) was fixed in supination of the forearm and dorsiflexion of the wrist. The dorsal Barton fracture (fracture of the articular surface of the distal radius with dislocation of the wrist) was fixed at the position of dorsiflexion of the wrist joint and pronation of the forearm, and the fixation of the volar Barton fracture was at the position of palmar flexion of the wrist joint and supination of the forearm. Periodically review the DR to understand the fracture location, and adjust the tightness of the small splint straps in time to maintain the effective fixation of the small splint.

2. Percutaneous needle fixation
For some patients with poor stability, simple plaster fixation cannot effectively maintain the fracture position, and percutaneous needle fixation is generally used. This treatment plan can be used as a separate external fixation method, and can be used in combination with plaster or external fixation brackets , which greatly increases the stability of the fractured end in the case of limited trauma, and has the characteristics of simple operation, easy removal, and less impact on the function of the patient's affected limb.
3. Other treatment options, such as open reduction, plate internal fixation, etc.
This type of plan can be used for patients with complex fracture types and high functional requirements. The treatment principles are anatomical reduction of fractures, support and fixation of displaced bone fragments, bone grafting of bone defects, and early assistance. Functional activities to restore the functional status before injury as soon as possible.
In general, for the vast majority of distal radius fractures, our hospital adopts conservative treatment methods such as manual reduction + plaster fixation + unique Honghui traditional Chinese medicine plaster application, etc., which can achieve good results.
PART 03
Precautions after reduction of distal radius fracture:
A. Pay attention to the degree of tightness when fixing distal radius fractures. The degree of fixation should be appropriate, neither too tight nor too loose. If it is fixed too tightly, it will affect the blood supply to the distal extremity, which may lead to severe ischemia of the distal extremity. If the fixation is too loose to provide fixation, bone shifting may occur again.
B. During the period of fracture fixation, it is not necessary to stop activities completely, but also need to pay attention to proper exercise. After the fracture has been immobilized for a period of time, some basic wrist movement will need to be added. Patients should insist on training every day, so as to ensure the exercise effect. In addition, for patients with fixers, the tightness of the fixers can be adjusted according to the exercise intensity.
C. After the distal radius fracture is fixed, pay attention to the feeling of the distal limbs and the color of the skin. If the distal limbs in the fixed area of the patient become cold and cyanotic, the sensation deteriorates, and the activities are severely limited, it is necessary to consider whether it is caused by too tight fixation, and it is necessary to return to the hospital for adjustment in time.
Yoyo
Sichuan Chenanhui Technology Co., Ltd
Tel/WhatsApp: +8615682071283
Email: liuyaoyao@medtechcah.com
Post time: Jan-06-2023





