




46% of rotational ankle fractures are accompanied by posterior malleolar fractures. The posterolateral approach for direct visualization and fixation of the posterior malleolus is a commonly used surgical technique, offering better biomechanical advantages compared to closed reduction and anteroposterior screw fixation. However, for larger posterior malleolar fracture fragments or posterior malleolar fractures involving the posterior colliculus of the medial malleolus, the posteromedial approach provides a better surgical view.
To compare the exposure range of the posterior malleolus, the tension on the neurovascular bundle, and the distance between the incision and the neurovascular bundle across three different posteromedial approaches, researchers conducted a cadaveric study. The results were recently published in the FAS journal. The findings are summarized as follows:
Currently, there are three main posteromedial approaches for exposing the posterior malleolus:
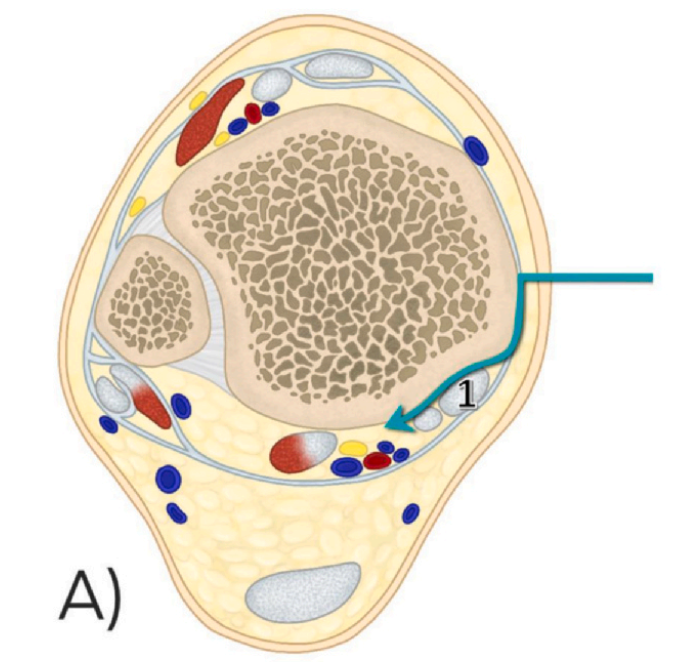
1. Medial Posteromedial Approach (mePM): This approach enters between the posterior edge of the medial malleolus and the tibialis posterior tendon (Figure 1 shows the tibialis posterior tendon).
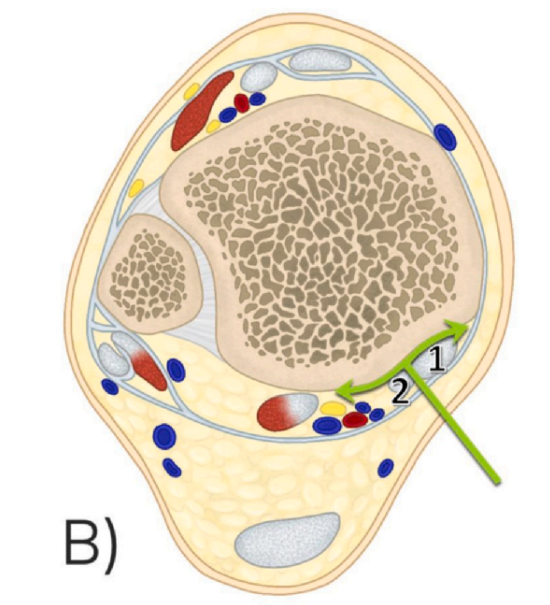
2. Modified Posteromedial Approach (moPM): This approach enters between the tibialis posterior tendon and the flexor digitorum longus tendon (Figure 1 shows the tibialis posterior tendon, and Figure 2 shows the flexor digitorum longus tendon).
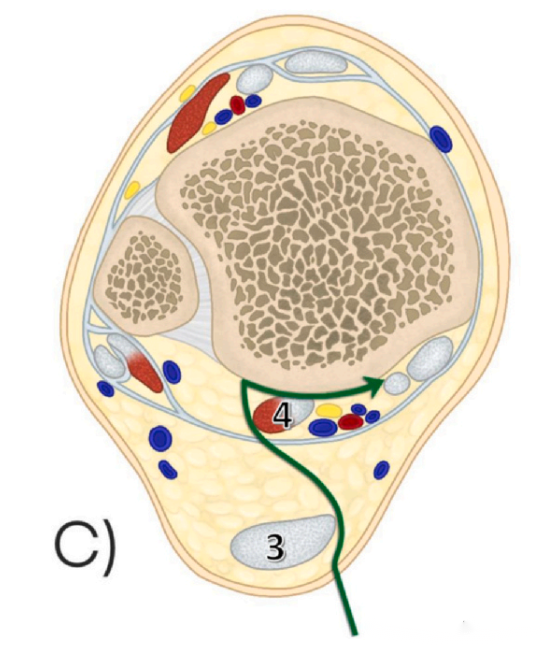
3. Posteromedial Approach (PM): This approach enters between the medial edge of the Achilles tendon and the flexor hallucis longus tendon (Figure 3 shows the Achilles tendon, and Figure 4 shows the flexor hallucis longus tendon).
Regarding the tension on the neurovascular bundle, the PM approach has a lower tension at 6.18N compared to the mePM and moPM approaches, indicating a lower likelihood of intraoperative traction injury to the neurovascular bundle.
In terms of the exposure range of the posterior malleolus, the PM approach also offers a greater exposure, allowing for 71% visibility of the posterior malleolus. In comparison, the mePM and moPM approaches allow for 48.5% and 57% exposure of the posterior malleolus, respectively.

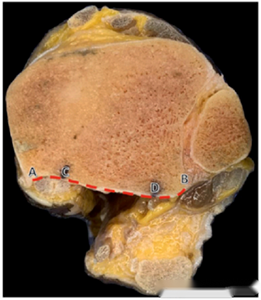
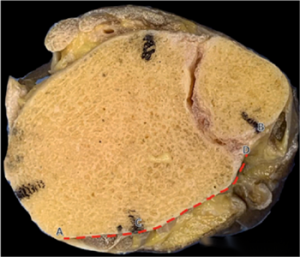
● The diagram illustrates the exposure range of the posterior malleolus for the three approaches. AB represents the overall range of the posterior malleolus, CD represents the exposed range, and CD/AB is the exposure ratio. From top to bottom, the exposure ranges for mePM, moPM, and PM are shown. It is evident that the PM approach has the largest exposure range.
Regarding the distance between the incision and the neurovascular bundle, the PM approach also has the greatest distance, measuring 25.5mm. This is greater than the mePM's 17.25mm and the moPM's 7.5mm. This indicates that the PM approach has the lowest likelihood of neurovascular bundle injury during surgery.
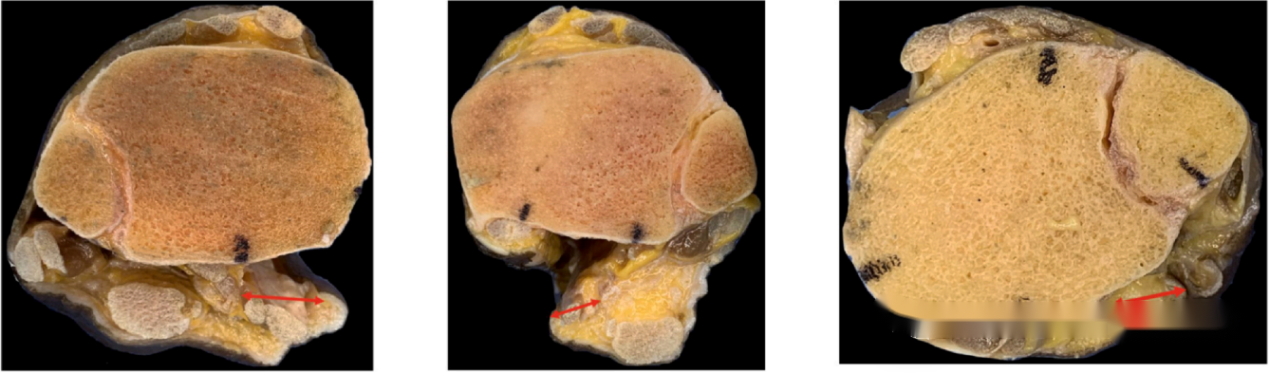
● The diagram shows the distances between the incision and the neurovascular bundle for the three approaches. From left to right, the distances for the mePM, moPM, and PM approaches are depicted. It is evident that the PM approach has the greatest distance from the neurovascular bundle.
Post time: May-31-2024





