




Proximal femoral fractures are commonly seen clinical injuries resulting from high-energy trauma. Due to the anatomical characteristics of the proximal femur, the fracture line often lies close to the articular surface and may extend into the joint, making it less suitable for intramedullary nail fixation. Consequently, a significant portion of cases still relies on fixation using a plate and screw system. However, the biomechanical features of eccentrically fixed plates pose a higher risk of complications such as lateral plate fixation failure, internal fixation rupture, and screw pull-out. The use of medial plate assistance for fixation, although effective, comes with the drawbacks of increased trauma, prolonged surgical time, heightened risk of postoperative infection, and added financial burden for the patients.
Given these considerations, in order to achieve a reasonable balance between the biomechanical drawbacks of lateral single plates and the surgical trauma associated with the use of both medial and lateral double plates, foreign scholars have adopted a technique involving lateral plate fixation with supplementary percutaneous screw fixation on the medial side. This approach has demonstrated favorable clinical outcomes.
After anesthesia, the patient is placed in a supine position.
Step 1: Fracture reduction. Insert a 2.0mm Kocher needle into the tibial tuberosity, traction to reset the limb length, and use a knee pad to correct the sagittal plane displacement.
Step 2: Placement of the lateral steel plate. After basic reduction by traction, directly approach the distal lateral femur, choose an appropriate length locking plate to maintain the reduction, and insert two screws at the proximal and distal ends of the fracture to maintain the fracture reduction. At this point, it is important to note that the two distal screws should be placed as close to the front as possible to avoid affecting the placement of the medial screws.
Step 3: Placement of medial column screws. After stabilizing the fracture with the lateral steel plate, use a 2.8mm screw-guided drill to enter through the medial condyle, with the needle point located in the middle or posterior position of the distal femoral block, diagonally outward and upward, penetrating the opposite cortical bone. After satisfactory fluoroscopy reduction, use a 5.0mm drill to create a hole and insert a 7.3mm cancellous bone screw.
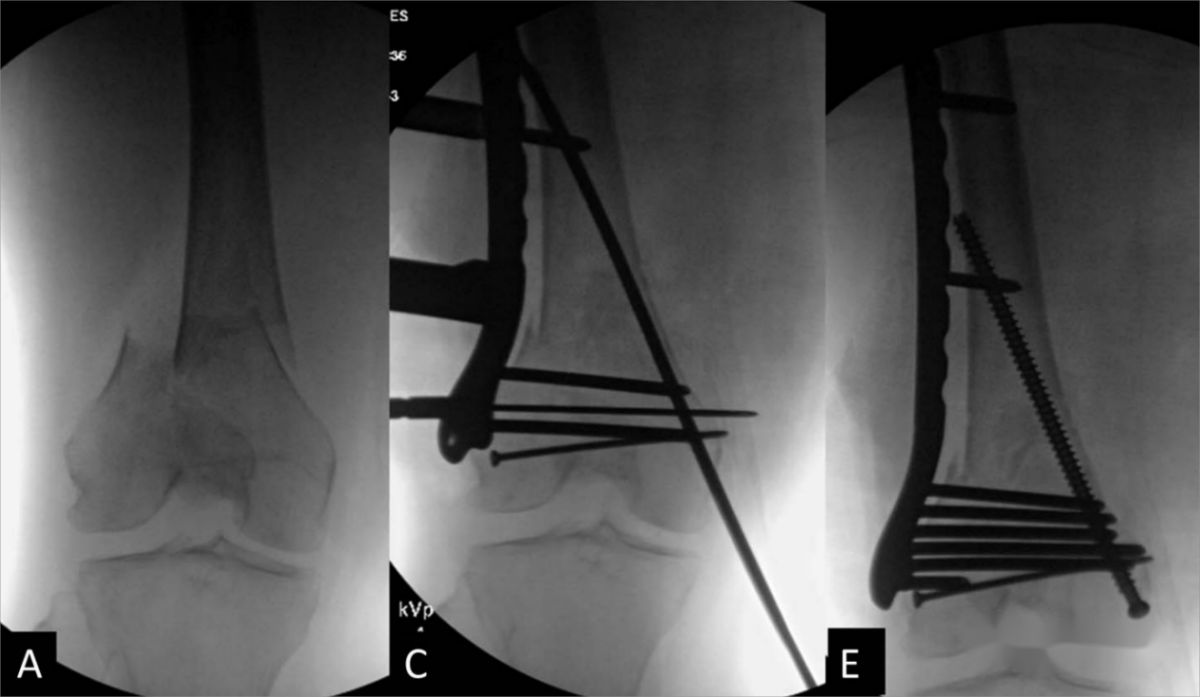
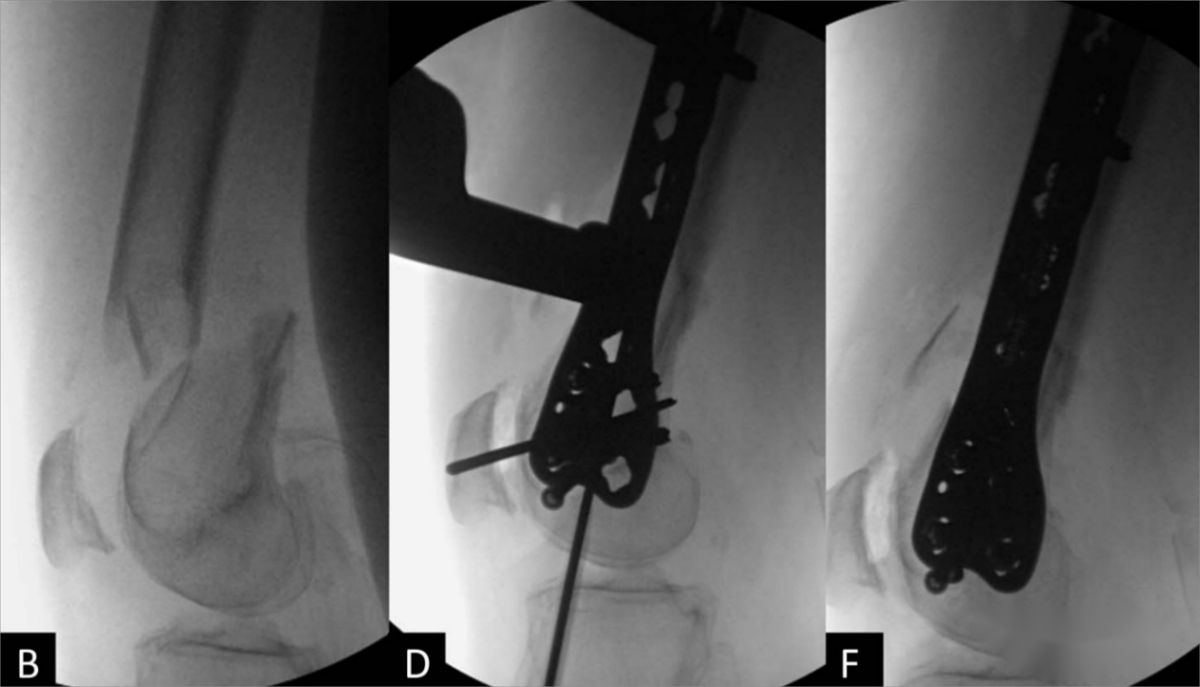
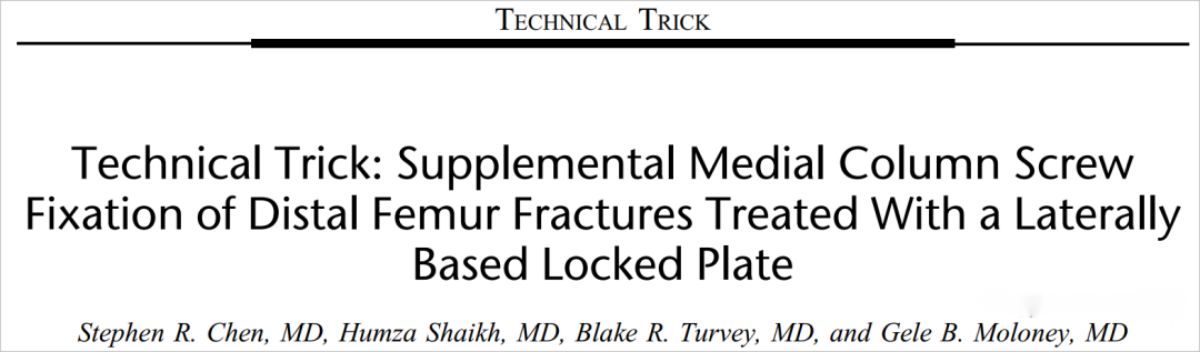
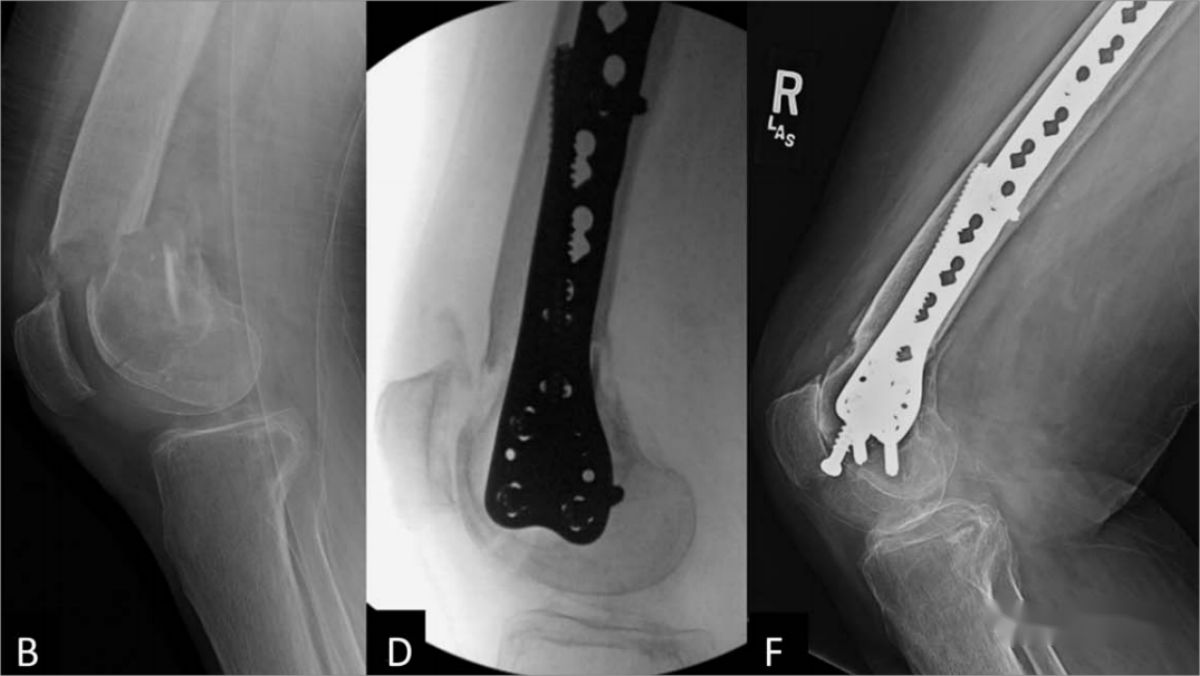
Diagram illustrating the process of fracture reduction and fixation. A 74-year-old female with a distal femoral intra-articular fracture (AO 33C1). (A, B) Preoperative lateral radiographs showing significant displacement of the distal femoral fracture; (C) After fracture reduction, an external lateral plate is inserted with screws securing both the proximal and distal ends; (D) Fluoroscopy image showing the satisfactory position of the medial guide wire; (E, F) Postoperative lateral and anteroposterior radiographs after insertion of the medial column screw.
During the reduction process, it is important to consider the following points:
(1) Use a guide wire with a screw. The insertion of medial column screws is relatively extensive, and using a guide wire without a screw may lead to a high angle during drilling through the medial condyle, making it prone to sliding.
(2) If the screws in the lateral plate effectively grasp the lateral cortex but fail to achieve effective dual cortex fixation, adjust the screw direction forward, allowing the screws to penetrate the anterior side of the lateral plate to achieve satisfactory dual cortex fixation.
(3) For patients with osteoporosis, inserting a washer with the medial column screw can prevent the screw from cutting into the bone.
(4) Screws at the distal end of the plate may obstruct the insertion of medial column screws. If screw obstruction is encountered during medial column screw insertion, consider withdrawing or repositioning the distal screws of the lateral plate, giving priority to the placement of the medial column screws.
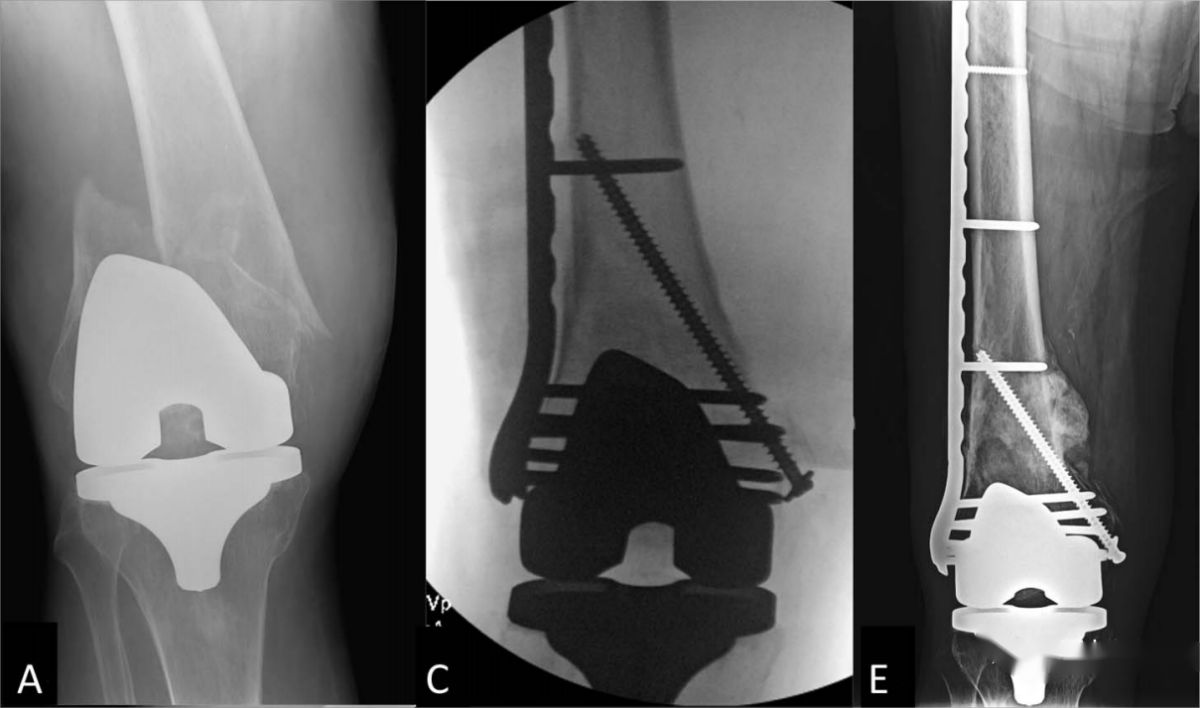
Case 2. Female patient, 76 years old, with a distal femoral extra-articular fracture. (A, B) Preoperative X-rays showing significant displacement, angular deformity, and coronal plane displacement of the fracture; (C, D) Postoperative X-rays in lateral and anteroposterior views demonstrating fixation with an external lateral plate combined with medial column screws; (E, F) Follow-up X-rays at 7 months postoperatively revealing excellent fracture healing with no signs of internal fixation failure.
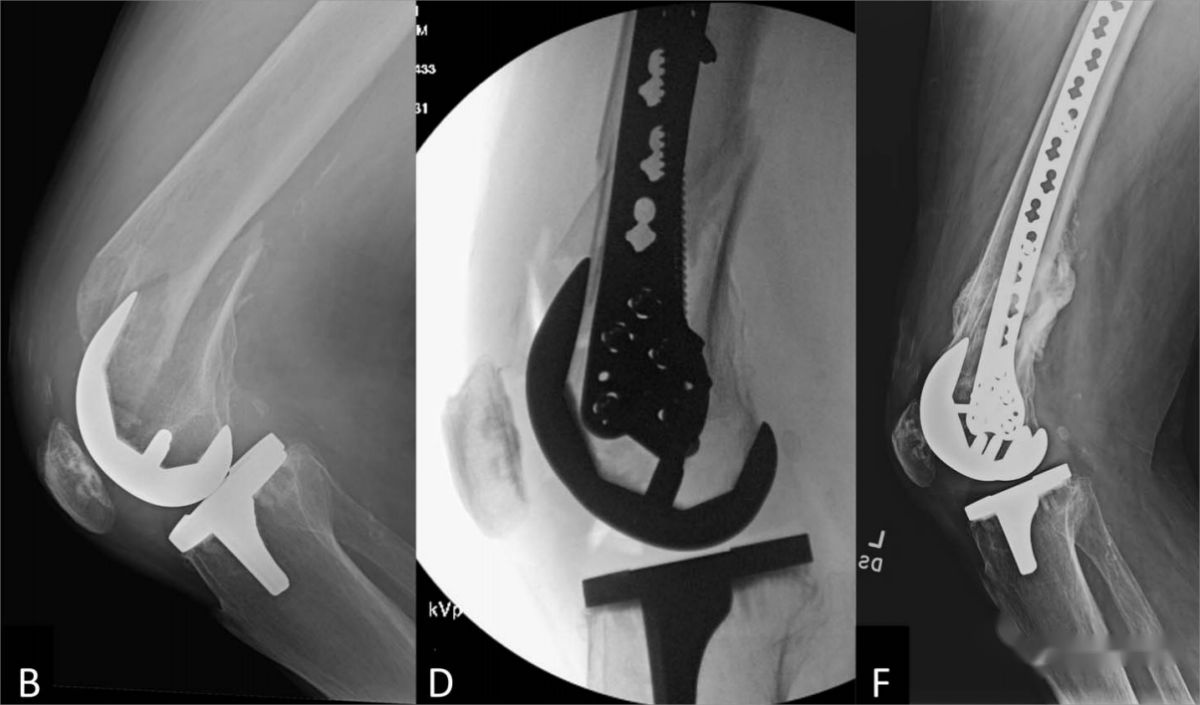
Case 3. Female patient, 70 years old, with a periprosthetic fracture around the femoral implant. (A, B) Preoperative X-rays showing a periprosthetic fracture around the femoral implant after total knee arthroplasty, with an extra-articular fracture and stable prosthetic fixation; (C, D) Postoperative X-rays illustrating fixation with an external lateral plate combined with medial column screws through an extra-articular approach; (E, F) Follow-up X-rays at 6 months postoperatively revealing excellent fracture healing, with the internal fixation in place.
Post time: Jan-10-2024





