




Ankle fractures are a common clinical injury. Due to the weak soft tissues around the ankle joint, there is significant blood supply disruption after injury, making healing challenging. Therefore, for patients with open ankle injuries or soft tissue contusions that cannot undergo immediate internal fixation, external fixation frames combined with closed reduction and fixation using Kirschner wires are usually employed for temporary stabilization. The definitive treatment is carried out in a second stage once the soft tissue condition has improved.
After a comminuted fracture of the lateral malleolus, there is a tendency for shortening and rotation of the fibula. If not corrected in the initial phase, managing the subsequent chronic fibular shortening and rotational deformity becomes more challenging in the second stage. To address this issue, foreign scholars have proposed a novel approach for the one-stage reduction and fixation of lateral malleolus fractures accompanied by severe soft tissue damage, aiming to restore both length and rotation.
Key Point 1: Correction of fibular shortening and rotation.
Multiple fractures or comminuted fractures of the fibula/lateral malleolus most commonly lead to fibular shortening and external rotation deformity:
▲ Illustration of fibular shortening (A) and external rotation (B).
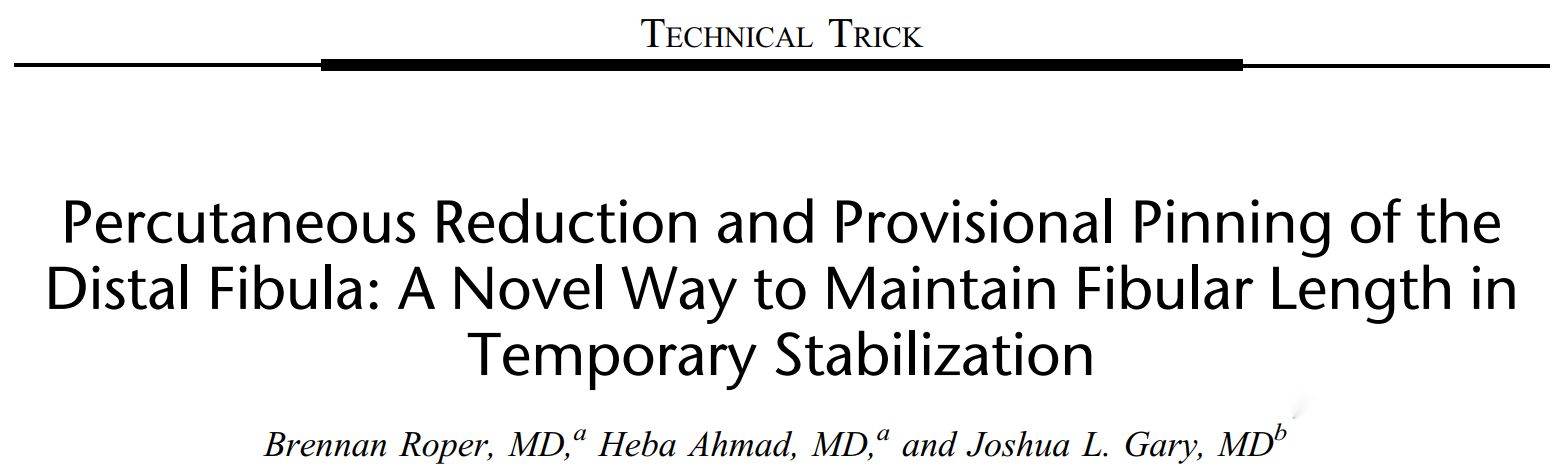
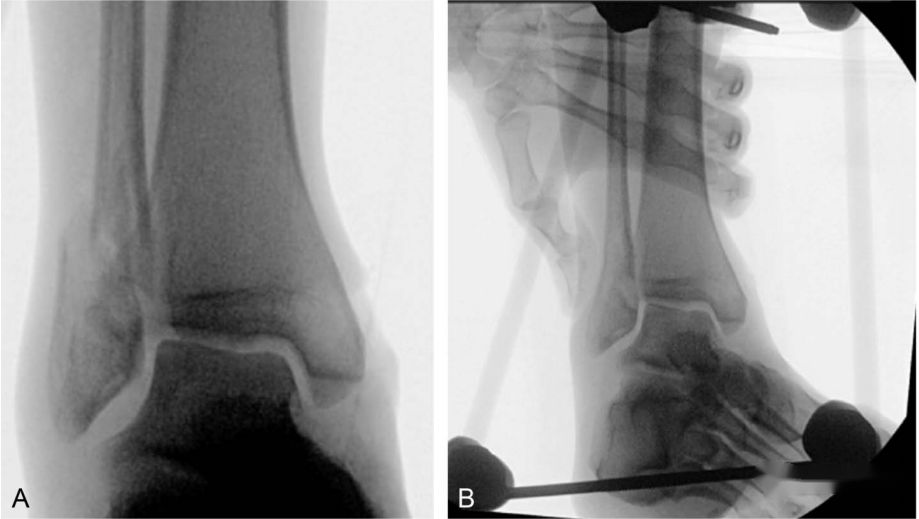
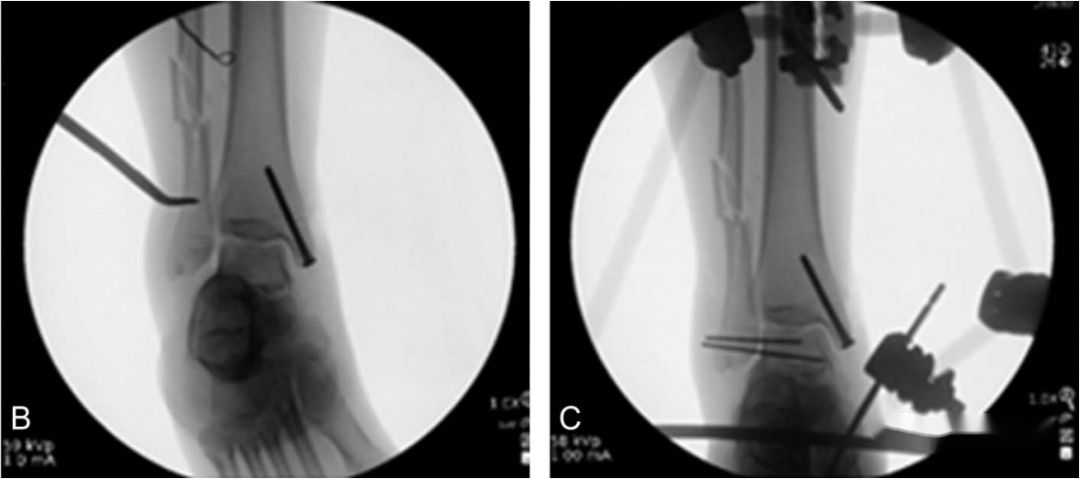
By manually compressing the fractured ends with fingers, it is usually possible to achieve the reduction of the lateral malleolus fracture. If direct pressure is insufficient for reduction, a small incision along the anterior or posterior edge of the fibula can be made, and a reduction forceps can be used to clamp and reposition the fracture.
▲ Illustration of external rotation of the lateral malleolus (A) and reduction after manual compression by fingers (B).
▲ Illustration of using a small incision and reduction forceps for assisted reduction.
Key Point 2: Maintenance of reduction.
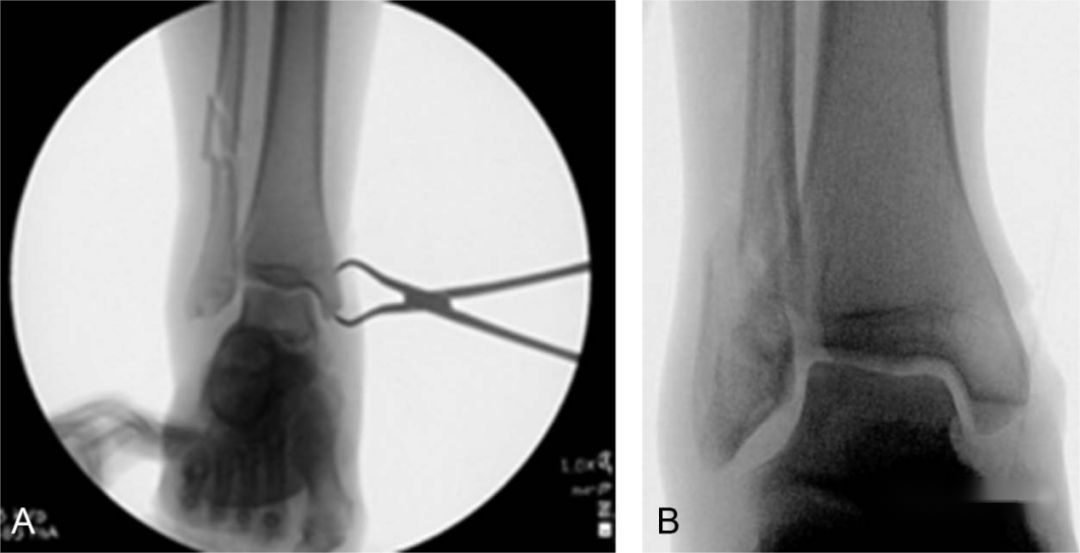
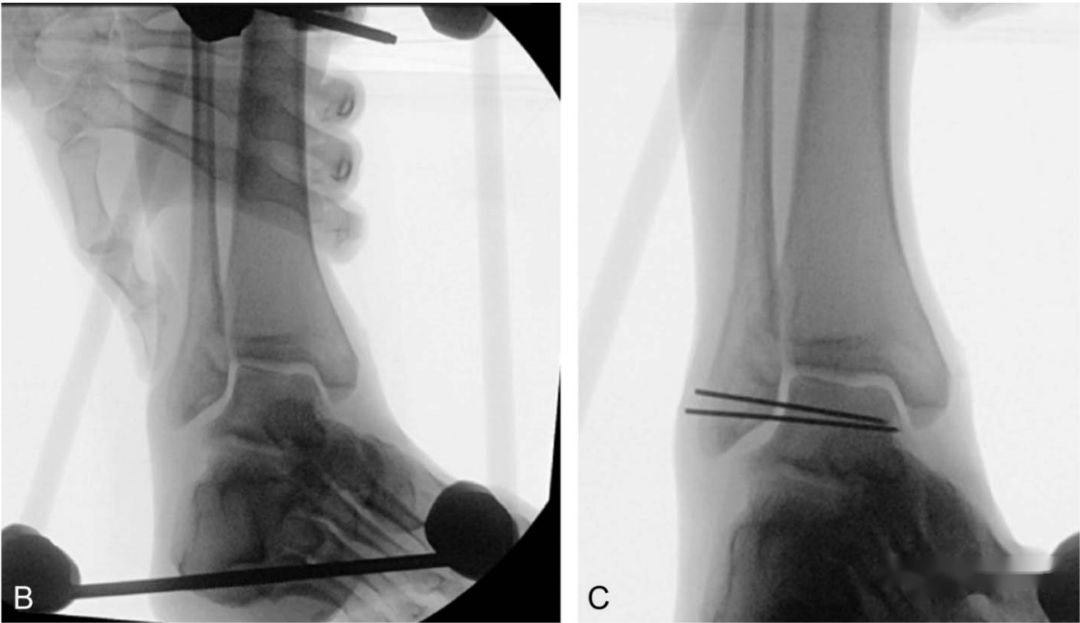
Following the reduction of a lateral malleolus fracture, two 1.6mm non-threaded Kirschner wires are inserted through the distal fragment of the lateral malleolus. They are placed directly to fix the lateral malleolus fragment to the tibia, maintaining the length and rotation of the lateral malleolus and preventing subsequent displacement during further treatment.
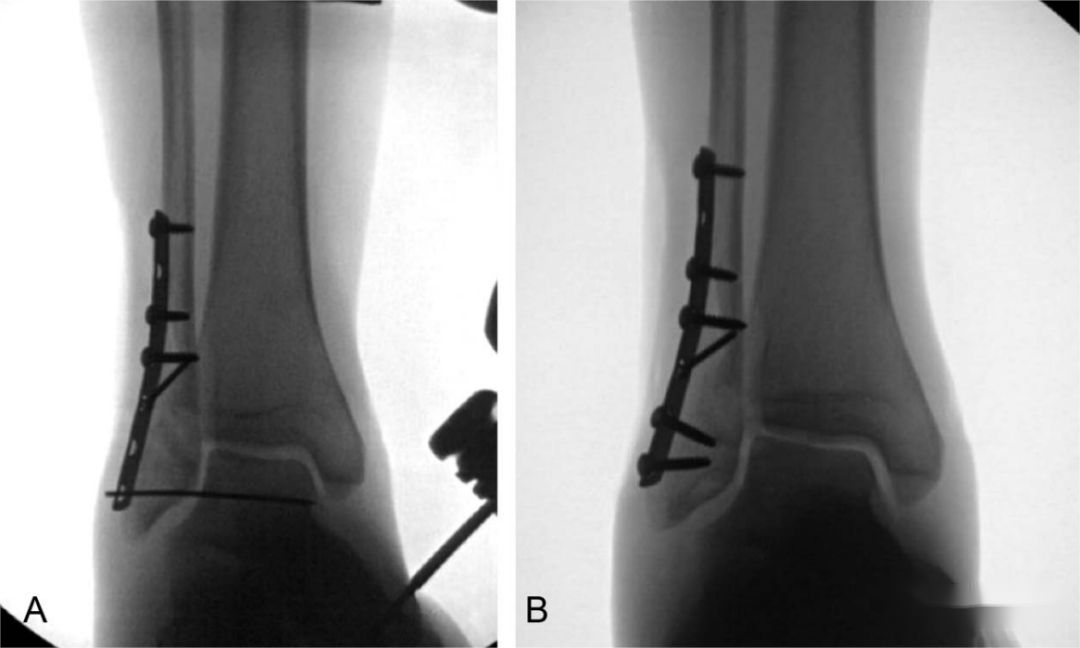
During the definitive fixation in the second stage, the Kirschner wires can be threaded out through the holes in the plate. Once the plate is securely fixed, the Kirschner wires are removed, and screws are then inserted through the Kirschner wire holes for additional stabilization.
Post time: Dec-11-2023





