




Navicular malunion occurs in approximately 5-15% of all acute fractures of the navicular bone, with navicular necrosis occurring in approximately 3%. Risk factors for navicular malunion include missed or delayed diagnosis, proximal proximity of the fracture line, displacement greater than 1 mm, and fracture with carpal instability. If left untreated, navicular osteochondral nonunion is often associated with traumatic arthritis, also known as navicular osteochondral nonunion with collapsing osteoarthritis.
Bone grafting with or without a vascularised flap can be used to treat navicular osteochondral nonunion. However, for patients with osteonecrosis of the proximal pole of the navicular bone, the results of bone grafting without a vascular tip are unsatisfactory, and the bone healing rate is only 40%-67%. In contrast, the healing rate of bone grafts with vascularised flaps can be as high as 88%-91%. The major vascularised bone flaps in clinical practice include 1,2-ICSRA-tipped distal radius flap, bone graft + vascular bundle implant, palmar radius flap, free iliac bone flap with vascularised tip, and medial femoral condylar bone flap (MFC VBG), etc. The results of bone grafting with vascularised tip are satisfactory. The free MFC VBG has been shown to be effective in the treatment of navicular fractures with metacarpal collapse, and the MFC VBG uses the articular branch of the descending knee artery as the main trophic branch. Compared with other flaps, the MFC VBG provides sufficient structural support to restore the normal shape of the navicular bone, especially in navicular fracture osteochondrosis with bowed back deformity (Figure 1). In the treatment of navicular osteochondral osteonecrosis with progressive carpal collapse, the 1,2-ICSRA-tipped distal radius flap has been reported to have a bone healing rate of only 40%, whereas the MFC VBG has a bone healing rate of 100%.
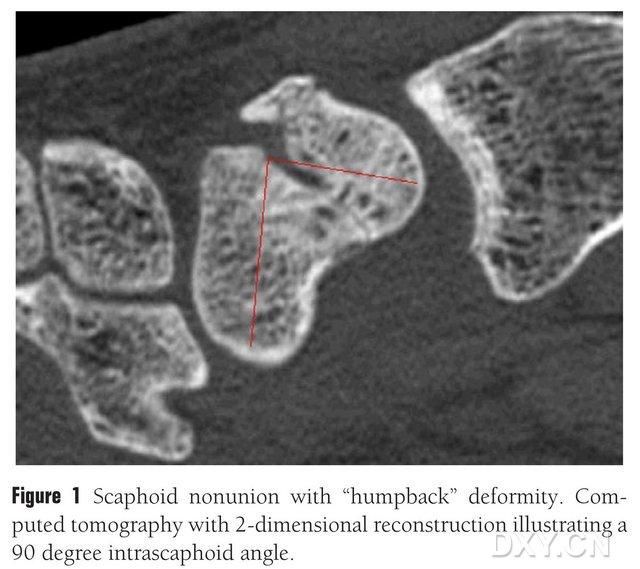
Figure 1. Fracture of the navicular bone with a "bowed back" deformity, CT shows the fracture block between the navicular bones at an angle of approximately 90°.
Preoperative preparation
After the physical examination of the affected wrist, imaging studies must be performed to assess the degree of wrist collapse. Plain radiographs are useful to confirm the location of the fracture, the degree of displacement, and the presence of resorption or sclerosis of the broken end. Posterior anterior images are used to assess for wrist collapse, dorsal instability of the wrist (DISI) using a modified wrist height ratio (height/width) of ≤1.52 or a radial lunate angle of greater than 15°. MRI or CT can help to diagnose malalignment of the navicular bone or osteonecrosis. Lateral radiographs or oblique sagittal CT of the navicular bone with a navicular angle >45° suggests shortening of the navicular bone, which is known as "bowed back deformity".MRI T1, T2 low signal suggests necrosis of the navicular bone, but MRI has no obvious significance in determining the healing of the fracture.
Indications and contraindications:
Navicular osteochondral nonunion with bowed back deformity and DISI; MRI shows ischemic necrosis of the navicular bone, intraoperative loosening of the tourniquet and observation of the fracture broken end of the navicular bone is still white sclerotic bone; the failure of the initial wedge bone grafting or screw internal fixation requires a large VGB structural bone grafting (>1cm3). preoperative or intraoperative findings of osteoarthritis of the radial carpal joint; if significant navicular malunion with collapsing osteoarthritis has occurred, then wrist denervation, navicular osteotomy, quadrangular fusion, proximal carpal osteotomy, total carpal fusion, etc., may be required; navicular malunion, proximal necrosis, but with normal navicular bone morphology (e.g., non-displaced navicular fracture with poor blood supply to the proximal pole); shortening of navicular malunion without osteonecrosis. (1,2-ICSRA can be used as a substitute for a distal radius flap).
Applied Anatomy
The MFC VBG is supplied by a number of small interosseous trophoblastic vessels (mean 30, 20-50), with the most abundant blood supply being posteriorly inferior to the medial femoral condyle (mean 6.4), followed by anteriorly superior (mean 4.9) (Fig. 2). These trophoblastic vessels were mainly supplied by the descending geniculate artery (DGA) and/or the superior medial geniculate artery (SMGA), which is a branch of the superficial femoral artery that also gives rise to articular, musculocutaneous, and/or saphenous nerve branches. the DGA originated from the superficial femoral artery proximal to the medial eminence of the medial malleolus, or at a distance of 13.7 cm proximal to the articular surface (10.5-17.5 cm), and the stability of the branching was 89% in the cadaveric specimens (Figure 3). The DGA originates from the superficial femoral artery at 13.7 cm (10.5 cm-17.5 cm) proximal to the medial malleolus fissure or proximal to the articular surface, with a cadaveric specimen showing 100% branching stability and a diameter of approximately 0.78 mm. Therefore, either the DGA or the SMGA is acceptable, although the former is more suitable for tibiae because of the length and diameter of the vessel.
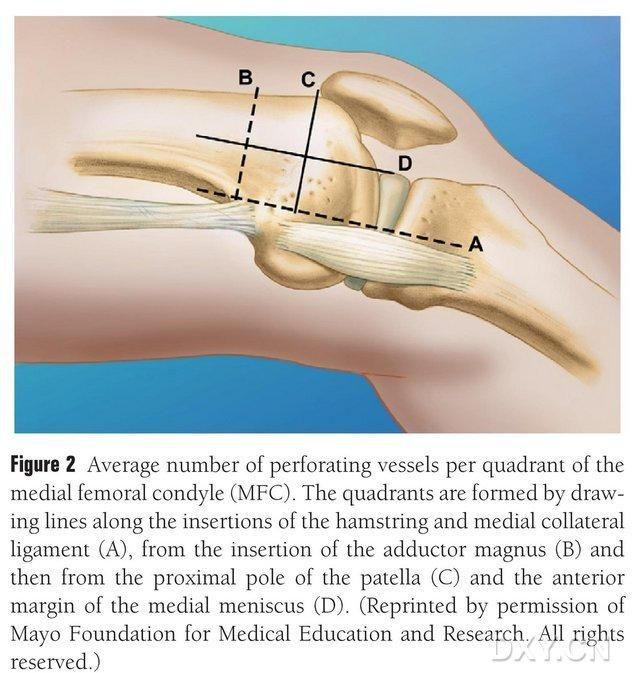
Fig. 2. Four-quadrant distribution of MFC trophoblast vessels along the horizontal line between the semitendinosus and the medial collateral ligament A, line of the greater trochanter B, line of the superior pole of the patella C, line of the anterior meniscus D.
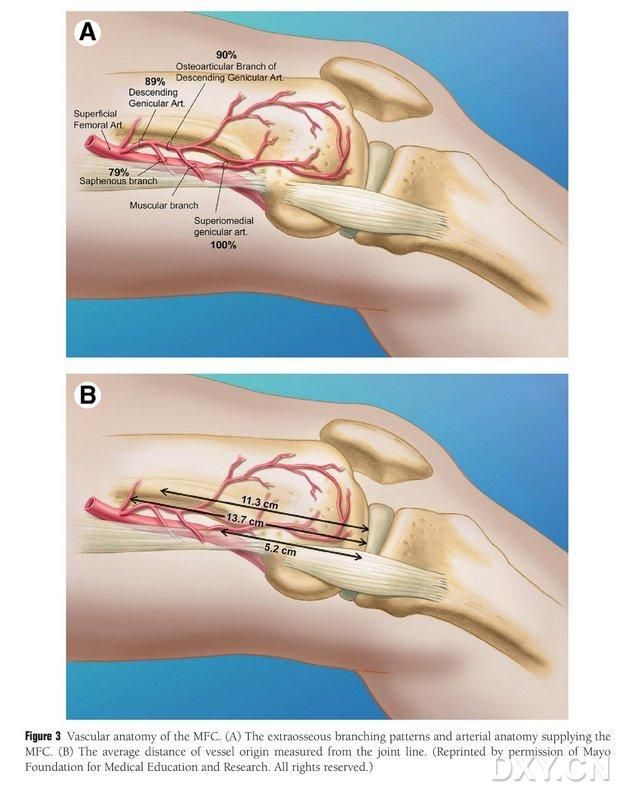
Figure 3. MFC vascular anatomy: (A) Extraosseous branches and MFC trophoblastic vascular anatomy, (B) Distance of vascular origins from the joint line
Surgical access
The patient is positioned under general anaesthesia in the supine position, with the affected limb placed on the hand surgery table. Generally, the donor bone flap is taken from the ipsilateral medial femoral condyle, so that the patient can move with crutches after surgery. The contralateral knee can also be chosen if there is a history of previous trauma or surgery on the same side of the knee. The knee is flexed and the hip is externally rotated, and tourniquets are applied to both the upper and lower extremities. The surgical approach was the extended Russe approach, with the incision starting 8 cm proximal to the transverse carpal tunnel and extending distally from the radial edge of the radial flexor carpi radialis tendon, and then folding at the transverse carpal tunnel towards the base of the thumb, ending at the level of the greater trochanter. The tendon sheath of the radial longissimus tendon is incised and the tendon is drawn ulnarly, and the navicular bone is exposed by sharp dissection along the radial lunate and radial navicular head ligaments, with careful separation of the peripheral soft tissues of the navicular bone to allow further exposure of the navicular bone (Figure 4). Confirm the area of nonunion, the quality of articular cartilage and the degree of ischaemia of the navicular bone. After loosening the tourniquet, observe the proximal pole of the navicular bone for punctate bleeding to determine whether there is ischaemic necrosis. If the navicular necrosis is not associated with radial carpal or intercarpal arthritis, MFC VGB may be used.
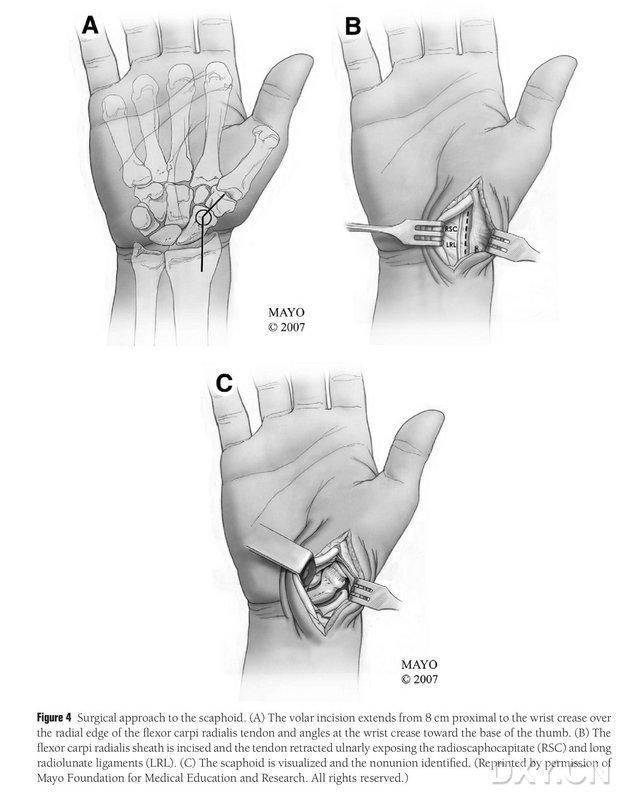
Figure 4. Navicular surgical approach: (A) The incision starts 8 cm proximal to the transverse carpal tunnel and extends the radial edge of the radial flexor carpi radialis tendon to the distal part of the incision, which is folded towards the base of the thumb at the transverse carpal tunnel. (B) The tendon sheath of the radial longissimus tendon is incised and the tendon is drawn ulnarly, and the navicular bone is exposed by sharp dissection along the radial lunate and radial navicular head ligaments. (C) Identify the area of the navicular osseous discontinuity.
A 15-20 cm long incision is made proximal to the knee joint line along the posterior border of the medial femoral muscle, and the muscle is retracted anteriorly to expose the MFC blood supply (Fig. 5).The MFC blood supply is generally supplied by the articular branches of the DGA and the SMGA, usually taking the larger joint branch of the DGA and the corresponding accompanying vein. The vascular pedicle is freed proximally, taking care to protect the periosteum and the trophoblastic vessels on the bony surface.
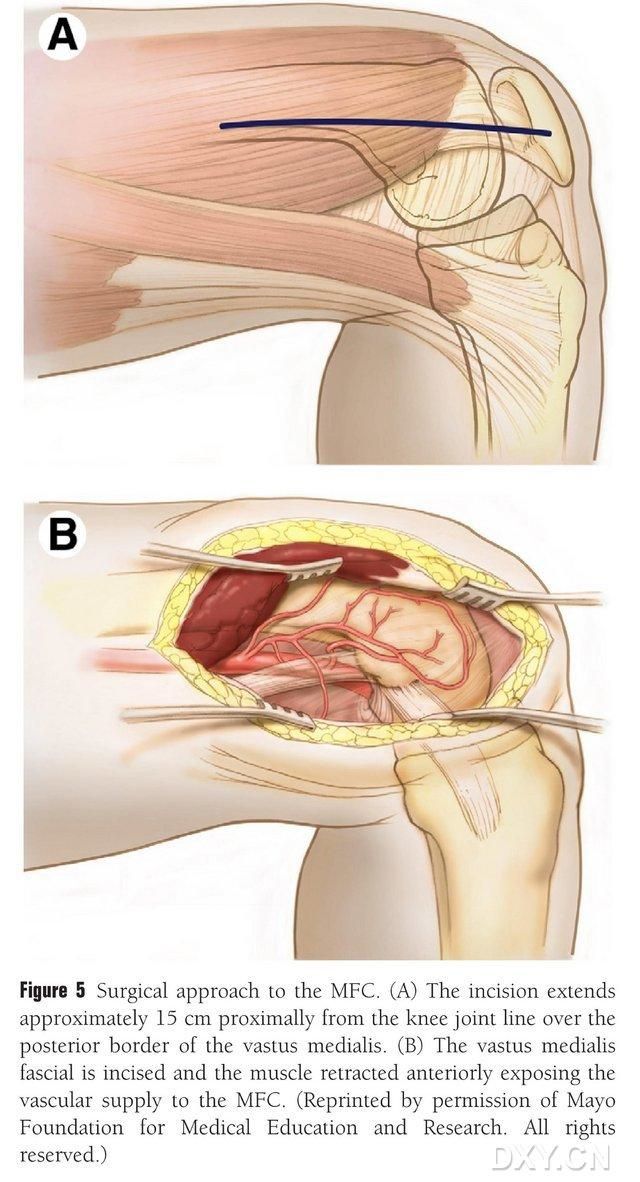
Figure 5. Surgical access to the MFC: (A) A 15-20 cm long incision is made proximally along the posterior border of the medial femoral muscle from the knee joint line. (B) The muscle is retracted anteriorly to expose the MFC blood supply.。
Preparation of the navicular bone
The navicular DISI deformity must be corrected and the area of the osteochondral bone graft prepared prior to implantation by flexing the wrist under fluoroscopy to restore a normal radial lunate angle (Figure 6). A 0.0625-foot (approximately 1.5-mm) Kirschner pin is drilled percutaneously from dorsal to metacarpal to fixate the radial lunate joint, and the navicular malunion gap is exposed when the wrist is straightened. The fracture space was cleared of soft tissue and further propped open with a plate spreader. A small reciprocating saw is used to flatten the bone and ensure that the implant flap resembles more of a rectangular structure than a wedge, which requires that the navicular gap be handled with a wider gap on the palmar side than on the dorsal side. After opening the gap, the defect is measured in three dimensions to determine the extent of the bone graft, which is usually 10-12 mm in length on all sides of the graft.
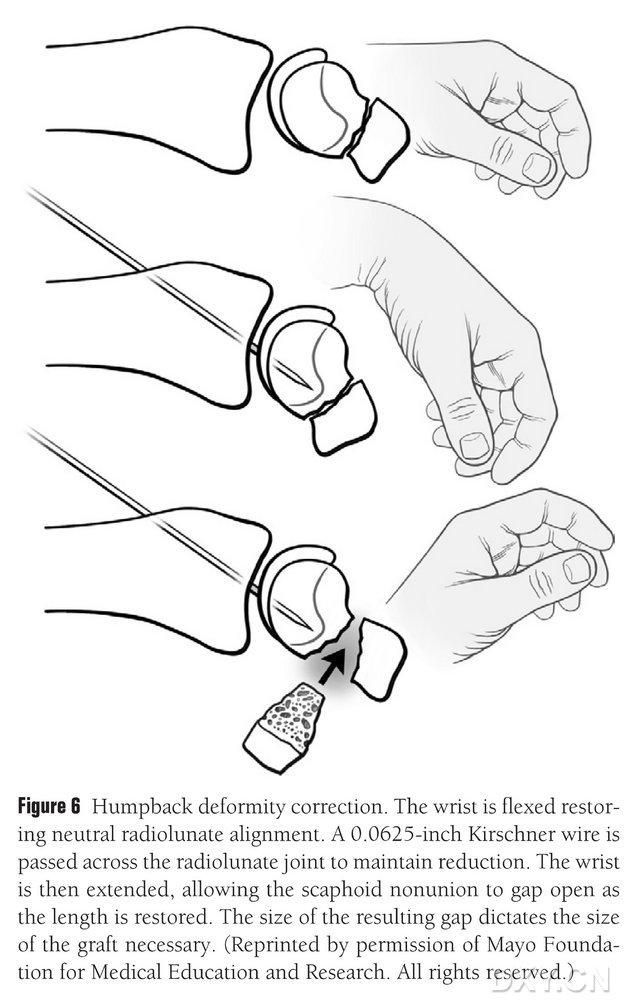
Figure 6. Correction of the bowed back deformity of the navicular, with fluoroscopic flexion of the wrist to restore normal radial-lunar alignment. A 0.0625-foot (approximately 1.5-mm) Kirschner pin is drilled percutaneously from dorsal to metacarpal to fixate the radial lunate joint, exposing the navicular malunion gap and restoring the normal height of the navicular bone when the wrist is straightened, with the size of the gap predicting the size of the flap that will need to be intercepted.
Osteotomy
The vascularised area of the medial femoral condyle is selected as the area of bone extraction, and the area of bone extraction is adequately marked. Be careful not to injure the medial collateral ligament. The periosteum is incised, and a rectangular bone flap of the appropriate size for the desired flap is cut with a reciprocating saw, with a second bone block cut at 45° along one side to ensure the integrity of the flap (Fig. 7). 7). Care should be taken not to separate the periosteum, cortical bone, and cancellous bone of the flap. The lower extremity tourniquet should be released to observe the blood flow through the flap, and the vascular pedicle should be freed proximally for at least 6 cm to allow for subsequent vascular anastomosis. If necessary, a small amount of cancellous bone can be continued within the femoral condyle. The femoral condylar defect is filled with a bone graft substitute, and the incision is drained and closed layer by layer.
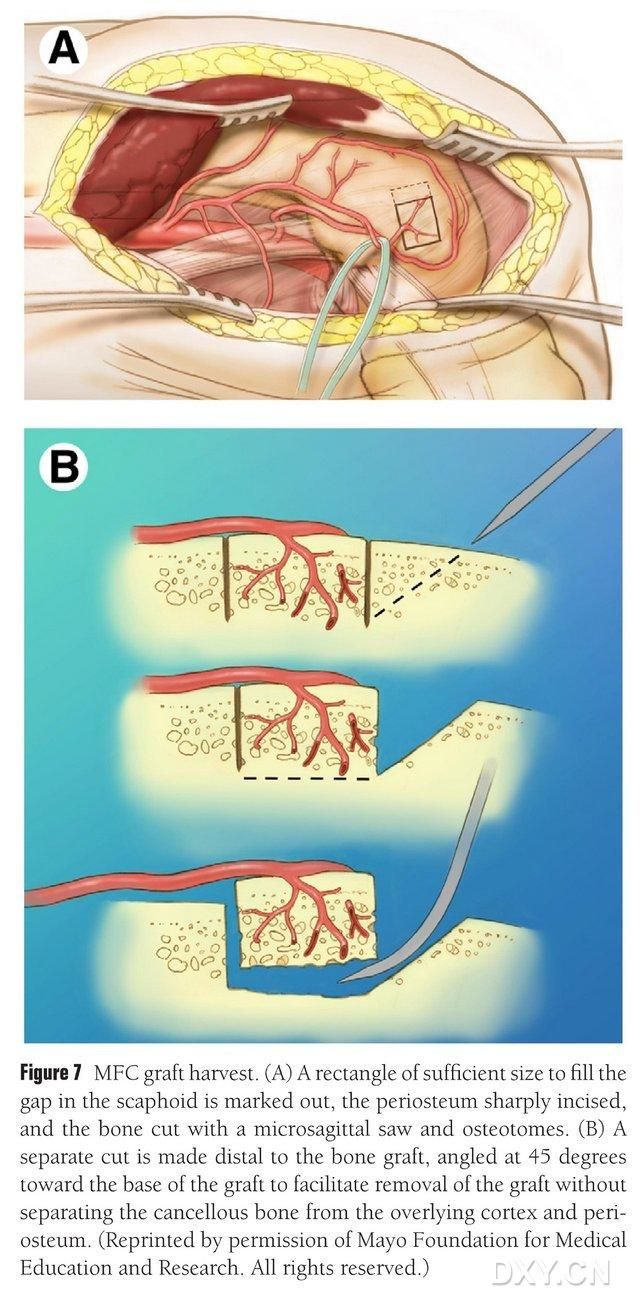
Figure 7. MFC bone flap removal. (A) The osteotomy area sufficient to fill the navicular space is marked, the periosteum is incised, and a rectangular bone flap of the appropriate size for the desired flap is cut with a reciprocating saw. (B) A second piece of bone is cut along one side at 45° to ensure the integrity of the flap.
Flap implantation and fixation
The bone flap is trimmed to the appropriate shape, taking care not to compress the vascular pedicle or strip the periosteum. The flap is gently implanted into the area of the navicular bone defect, avoiding percussion, and fixed with hollow navicular screws. Care was taken to ensure that the palmar margin of the implanted bone block was flush with the palmar margin of the navicular bone or that it was slightly depressed to avoid impingement. Fluoroscopy was performed to confirm navicular bone morphology, line of force and screw position. Anastomose the vascular flap artery to the radial artery end to side and the venous tip to the radial artery companion vein end to end (Figure 8). The joint capsule is repaired, but the vascular pedicle is avoided.
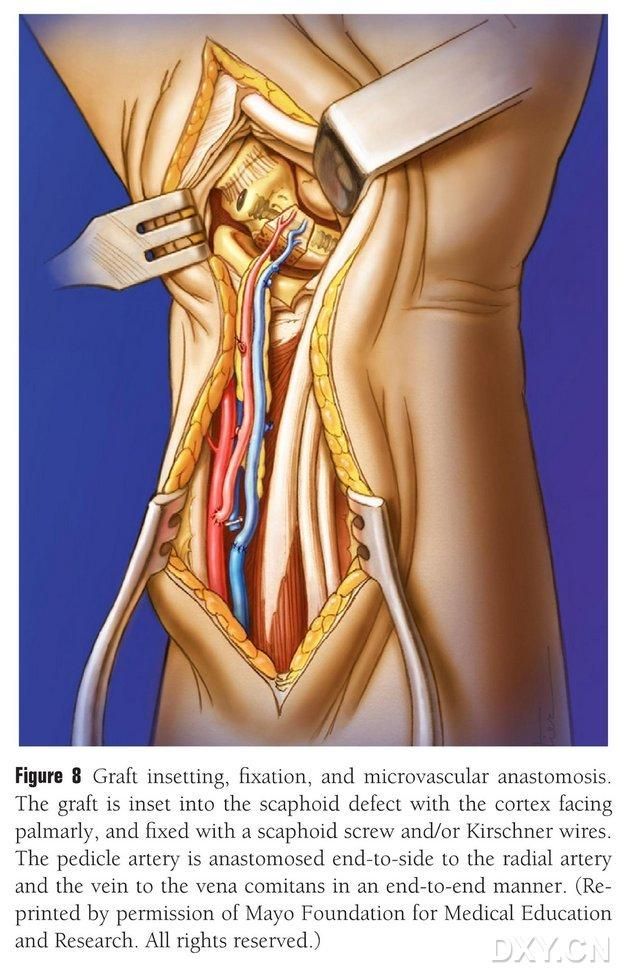
Figure 8. Bone flap implantation, fixation, and vascular anastomosis. The bone flap is gently implanted into the area of the navicular bone defect and fixed with hollow navicular screws or Kirschner pins. Care is taken that the metacarpal margin of the implanted bone block is flush with the metacarpal margin of the navicular bone or mildly depressed to avoid impingement. Anastomosis of the vascular flap artery to the radial artery was performed end to end, and the vein tip to the radial artery companion vein was performed end to end.
Postoperative rehabilitation
Oral aspirin 325 mg per day (for 1 month), postoperative weight-bearing of the affected limb is permitted, knee braking can reduce the discomfort of the patient, depending on the patient's ability to move at the right time. Contralateral support of a single crutch can reduce pain, but long-term support of crutches is not necessary. The stitches were removed 2 weeks after surgery and the Muenster or long arm to thumb cast was kept in place for 3 weeks. After that, the short arm to thumb cast is used until the fracture heals. X-rays are taken at 3-6 week intervals, and fracture healing is confirmed by CT. Afterwards, active and passive flexion and extension activities should be started gradually, and the intensity and frequency of exercise should be increased gradually.
Major complications
The main complications of the knee joint include knee pain or nerve injury. Knee pain mainly occurred within 6 weeks after surgery, and no sensory loss or painful neuroma due to saphenous nerve injury was found. The main wrist complications included refractory bone nonunion, pain, joint stiffness, weakness, progressive osteoarthritis of the radial wrist or intercarpal bones, and the risk of periosteal heterotopic ossification has also been reported.
Free Medial Femoral Condyle Vascularised Bone Grafting for Scaphoid Nonunions with Proximal Pole Avascular Necrosis and Carpal Collapse
Post time: May-28-2024





