




Over the past few decades, the incidence of proximal humeral fractures (PHFs) has increased by more than 28%, and the surgical rate has increased by more than 10% in patients aged 65 years and older. Obviously, decreased bone density and increased number of falls are major risk factors in the increasing elderly population. Although various surgical treatments are available to manage displaced or unstable PHFs, there is no consensus on the best surgical approach for the elderly. The development of angle stabilization plates has provided a treatment option for the surgical treatment of PHFs, but the high complication rate of up to 40% must be considered. The most commonly reported are adduction collapse with screw dislodgement and avascular necrosis (AVN) of the humeral head.
Anatomical reduction of the fracture, restoration of humeral moment, and accurate subcutaneous fixation of the screw can reduce such complications. Screw fixation is often difficult to achieve due to the compromised bone quality of the proximal humerus caused by osteoporosis. To address this problem, strengthening the bone-screw interface with poor bone quality by applying polymethylmethacrylate (PMMA) bone cement around the screw tip is a new approach to improve the fixation strength of the implant.
The current study aimed to evaluate and analyze the radiographic results of PHFs treated with angled stabilization plates and additional screw tip augmentation in patients older than 60 years.
Ⅰ.Material and Method
A total of 49 patients underwent angle-stabilized plating and additional cement augmentation with screws for PHFs, and 24 patients were included in the study based on the inclusion and exclusion criteria.
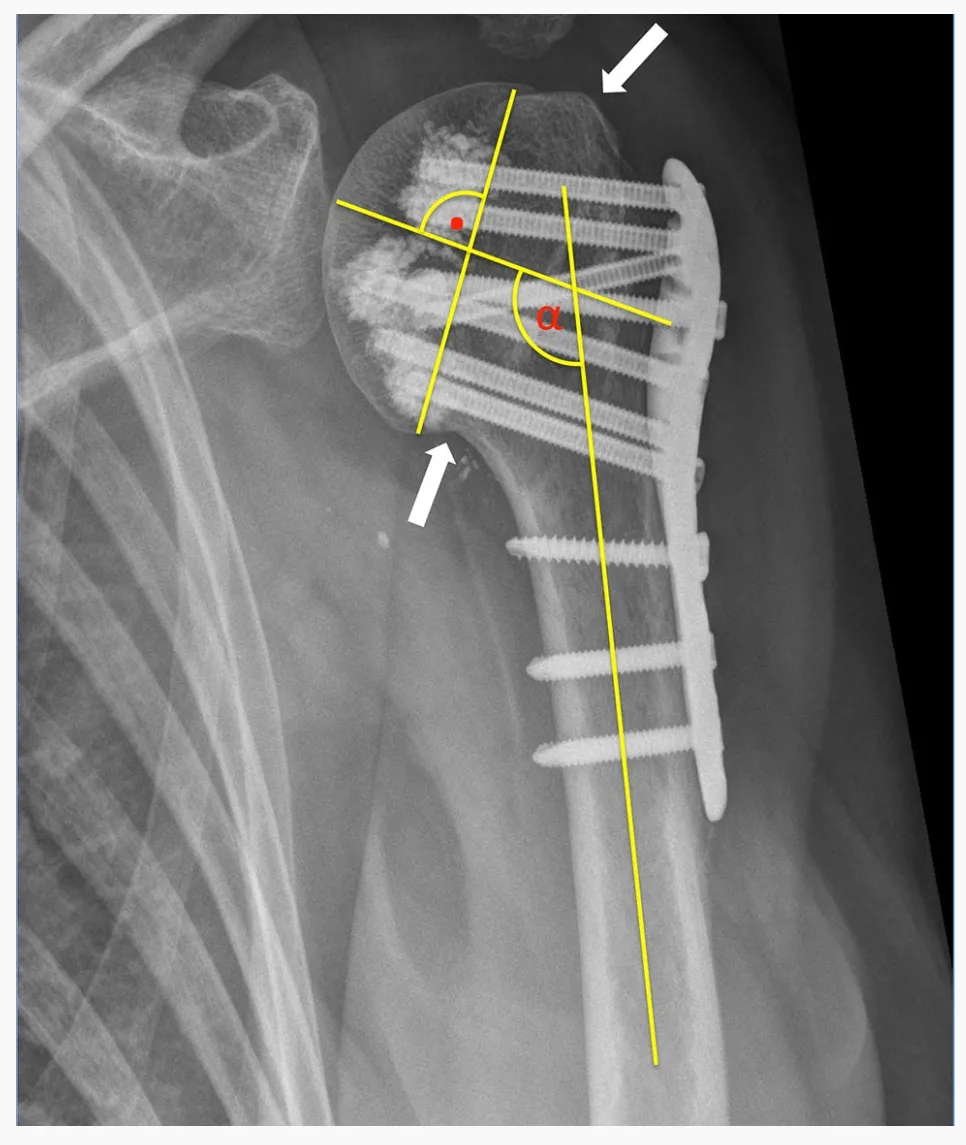
All 24 PHFs were classified using the HGLS classification system introduced by Sukthankar and Hertel using preoperative CT scans. Preoperative radiographs as well as postoperative plain radiographs were evaluated. Adequate anatomic reduction of the fracture was considered achieved when the tuberosity of the humeral head was re-reduced and showed less than 5 mm of gap or displacement. Adduction deformity was defined as an inclination of the humeral head relative to the humeral shaft of less than 125° and valgus deformity was defined as more than 145°.
Primary screw penetration was defined as the screw tip penetrating the border of the medullary cortex of the humeral head. Secondary fracture displacement was defined as a displacement of the reduced tuberosity of more than 5 mm and/or a change of more than 15° in the inclination angle of the head fragment on the follow-up radiograph compared with the intraoperative radiograph.
All surgeries were performed via a deltopectoralis major approach. Fracture reduction and plate positioning were performed in a standard manner. Screw-cement augmentation technique used 0.5 ml of cement for screw tip augmentation.
Immobilization was performed postoperatively in a custom arm sling for the shoulder for 3 weeks. Early passive and assisted active motion with pain modulation was initiated 2 days postoperatively to achieve full range of motion (ROM).
Ⅱ.Consequence.
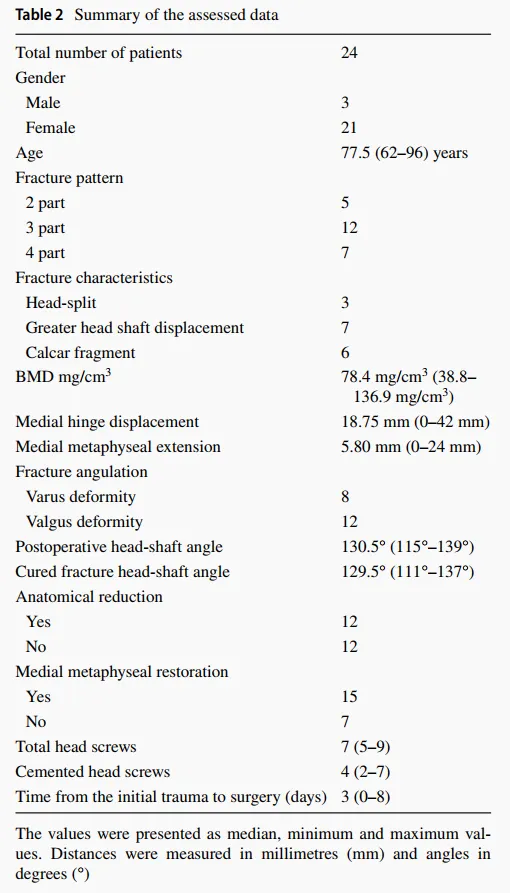
Results: Twenty-four patients were included, with a median age of 77.5 years (range, 62-96 years). Twenty-one were female and three were male. Five 2-part fractures, 12 3-part fractures, and seven 4-part fractures were surgically treated using angled stabilization plates and additional screw-cement augmentation. Three of the 24 fractures were humeral head fractures. Anatomic reduction was achieved in 12 of the 24 patients; complete reduction of the medial cortex was achieved in 15 of the 24 patients (62.5%). At 3 months after surgery, 20 of the 21 patients (95.2%) had achieved fracture union, except for 3 patients who required early revision surgery.

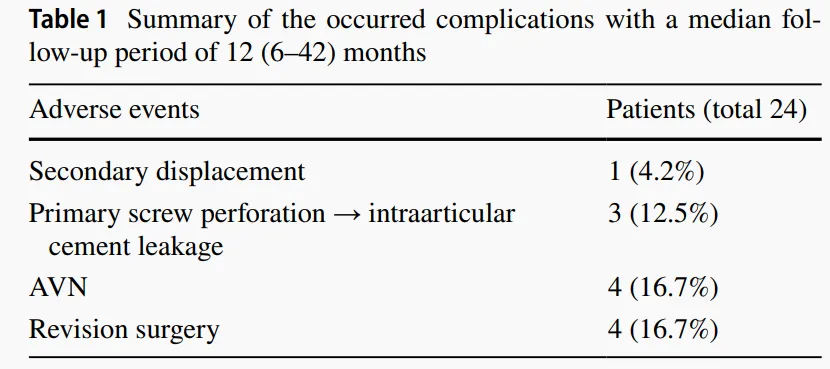
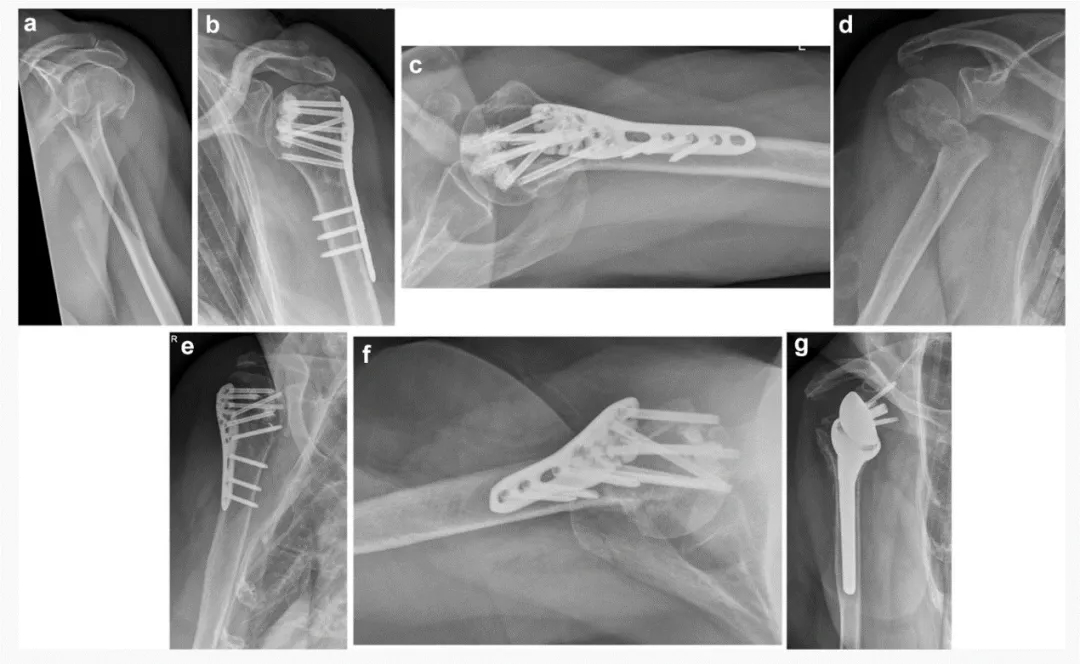
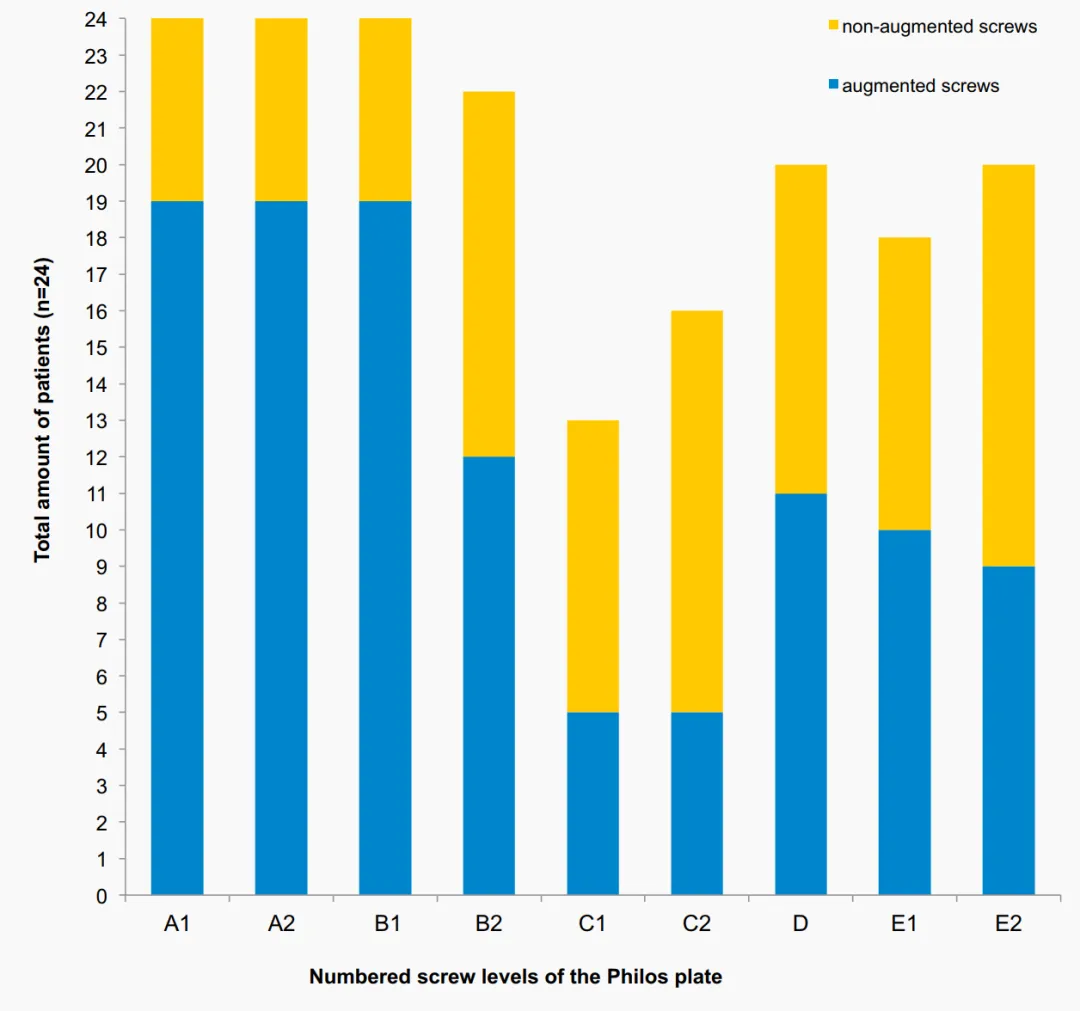
One patient developed early secondary displacement (posterior rotation of the humeral head fragment) 7 weeks after surgery. Revision was performed with a reverse total shoulder arthroplasty 3 months after surgery. Primary screw penetration due to small intraarticular cement leakage (without major erosion of the joint) was observed in 3 patients (2 of whom had humeral head fractures) during postoperative radiographic follow-up. Screw penetration was detected in the C layer of the angle stabilization plate in 2 patients and in the E layer in another (Fig. 3). 2 of these 3 patients subsequently developed avascular necrosis (AVN). The patients underwent revision surgery due to the development of AVN (Tables 1, 2).
Ⅲ.Discussion.
The most common complication in proximal humeral fractures (PHFs), besides the development of avascular necrosis (AVN), is screw dislodgement with subsequent adduction collapse of the humeral head fragment. This study found that cement-screw augmentation resulted in a union rate of 95.2% at 3 months, secondary displacement rate of 4.2%, AVN rate of 16.7%, and total revision rate of 16.7%. Cement augmentation of screws resulted in a secondary displacement rate of 4.2% without any adduction collapse, which is a lower rate compared to the approximately 13.7-16% with conventional angled plate fixation. We strongly recommend that efforts be made to achieve adequate anatomic reduction, especially of the medial humeral cortex in angled plate fixation of PHFs. Even if additional screw tip augmentation is applied, well-known potential failure criteria must be considered.
The overall revision rate of 16.7% using screw tip augmentation in this study is within the lower range of previously published revision rates for traditional angular stabilization plates in PHFs, which have shown revision rates in the elderly population ranging from 13% to 28%. No wait. The prospective, randomized, controlled multicenter study conducted by Hengg et al. did not show the benefit of cement screw augmentation. Among a total of 65 patients who completed 1-year follow-up, mechanical failure occurred in 9 patients and 3 in the augmentation group. AVN was observed in 2 patients (10.3%) and in 2 patients (5.6%) in the non-enhanced group. Overall, there were no significant differences in the occurrence of adverse events and clinical outcomes between the two groups. Although these studies focused on clinical and radiological outcomes, they did not evaluate radiographs in as much detail as this study. Overall, radiologically detected complications were similar to those in this study. None of these studies reported intra-articular cement leakage, except for the study by Hengg et al., who observed this adverse event in one patient. In the present study, primary screw penetration was observed twice at level C and once at level E, with subsequent intra-articular cement leakage without any clinical relevance. Contrast material was injected under fluoroscopic control before cement augmentation was applied to each screw. However, different radiographic views at different arm positions should be performed and evaluated more carefully to rule out any primary screw penetration before cement application. Furthermore, cement reinforcement of screws at level C (screw divergent configuration) should be avoided due to the higher risk of main screw penetration and subsequent cement leakage. Cement screw tip augmentation is not recommended in patients with humeral head fractures due to the high potential for intraarticular leakage observed in this fracture pattern (observed in 2 patients).
VI. Conclusion.
In the treatment of PHFs with angle-stabilized plates using PMMA cement, cement screw tip augmentation is a reliable surgical technique that enhances the fixation of the implant to the bone, resulting in a low secondary displacement rate of 4.2% in osteoporotic patients. Compared with the existing literature, an increased incidence of avascular necrosis (AVN) was observed mainly in severe fracture patterns and this must be taken into account. Before cement application, any intraarticular cement leakage must be carefully excluded by contrast medium administration. Due to the high risk of intraarticular cement leakage in humeral head fractures, we do not recommend cement screw tip augmentation in this fracture.
Post time: Aug-06-2024





