




After fracture, the bone and surrounding tissues are damaged, and there are different treatment principles and methods according to the degree of injury. Before treating all fractures, it is essential to determine the extent of the injury.
Soft tissue injuries
I.Classification
Closed fractures
Soft tissue injuries are graded from mild to severe, usually using the Tscherne method (Fig. 1)
Grade0 injury: Minor soft tissue injury
Grade1 injury: superficial abrasion or contusion of soft tissue covering the fracture site
Grade2 injury: significant muscle contusion or contaminated skin contusion or both
Grade3 injury: Severe soft tissue injury with severe displacement, crushing, compartment syndrome, or vascular injury
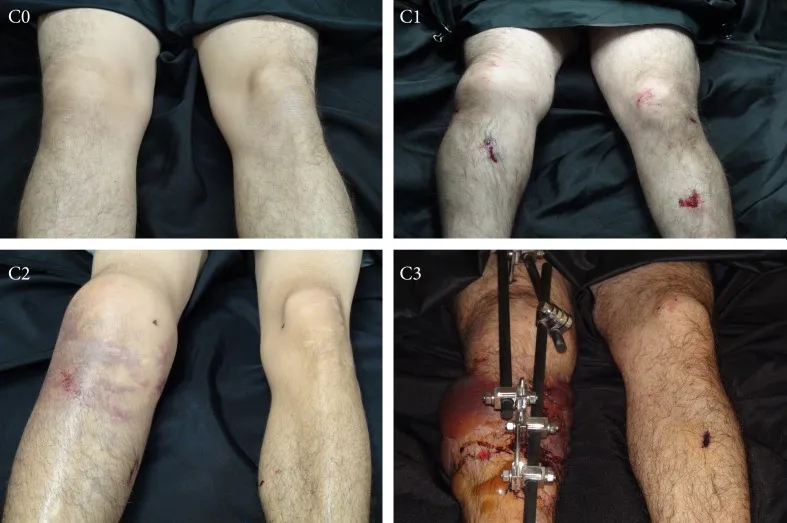
Figure1:Tscherne Classification
Open Fracture
Because the fracture is communicative to the outside world, the degree of soft tissue damage is related to the amount of energy experienced by the limb during the trauma, and the Gustilo classification is usually used (Figure 2)

Figure2:GustiloClassification
Type I: Clean wound length < 1 cm, small muscle damage, no obvious periosteal exfoliation Type II: wound length > 1 cm, no obvious soft tissue damage, flap formation or avulsion injury
Type III: Wound range includes skin, muscle, periosteum, and bone, with more extensive trauma, including special types of gunshot wounds and farm injuries
Type IIIa: Widespread contamination and/or presence of deep soft tissue lesions, soft tissues with adequate coverage of bone and neurovascular structures
Type IIIb: with extensive soft tissue damage, Rotational or free muscle metastases are required during treatment to achieve coverage
Type IIIc: Open fractures with vascular damage requiring manual repair Gustilo classification tends to become progressively worse over time, with changes in injury grade noted during repair.
II.Injury management
Wound healing requires oxygenation, activation of cellular mechanisms, cleansing of wounds free of contaminated and necrotic tissue. There are four main stages of healing: coagulation (minutes); inflammatory phase (hours); granulation tissue stage (days counted); Scar tissue formation period (weeks).
Staging of treatment
Acute phase: wound irrigation, debridement, bone reconstruction, and recovery of range of motion
(1)Evaluate the extent of soft tissue injury and related neurovascular injury
(2)Use a large amount of isotonic fluid for pulsating irrigation in the operating room to remove necrotic tissue and foreign bodies
(3)Debridement is carried out every 24~48 hours to remove all foreign bodies and necrotic tissues from the wound until the wound can be closed or completely covered (4) The open wound is appropriately extended, the deep tissue is fully exposed, and effective evaluation and debridement are carried out .
(5)The free fracture end is retracted into the wound; Small deactivated cortex is removed to examine and clean the bone marrow cavity
Reconstruction: dealing with the sequelae of trauma (delayed union, nonunion, deformity, infection)
Convalescence: Psychological, social, and occupational regression of the patient
Type of wound closure and coverage
Early wound closure or coverage (3~5 days) can achieve satisfactory treatment results: (1) primary closure
(2)delayed closure
(3)secondary closure
(4)medium-thick flap transplantation
(5)voluntary flap (adjacent digital flap)
(6)vascular pedicle flap (gastrocnemius flap)
(7) free flap (Fig. 3)

Figure3:Partial views of free transplants are often provided
Bone damage
I.Fracture line direction
Transverse: Load pattern of a transverse fracture caused by tension
obliquely: Load mode of a pressure due to a diagonal fracture
Spiral: Load pattern of a torsional fracture due to a spiral fracture
II.Fractures
Classification according to fractures, fracture types, etc. (Fig. 4)
Comminuted fractures are fractures with 3 or more living bone fragments, usually resulting from a high-energy injury.
Pathological fracture fracture line fracture occurs in the area of bone deterioration of the previous disease, including: primary bone tumor, bone metastases, osteoporosis, metabolic bone disease, etc
Incomplete fractures do not break into separate pieces of bone
Segmental fractures with distal, middle, and proximal fracture fragments. The middle segment is affected by the blood supply, usually as a result of a high-energy injury, with soft tissue detachment from the bone, causing problems with bone healing.
Fractures with bone defects, open fractures with bone fragments, or trauma-inactive fractures that need to be cleared, or severe comminuted fractures that result in bone defects.
Fractures with butterfly bone fragments are similar to segmental fractures in that they do not involve the entire cross-section of the bone and are usually the result of bending violence.
Stress fractures are caused by repeated loads and often occur in the calcaneus and tibia.
Avulsion fractures cause a fracture of the bone's insertion point when a tendon or ligament is stretched.
Compression fractures are fractures in which the bone fragments are squeezed, usually by axial loads.
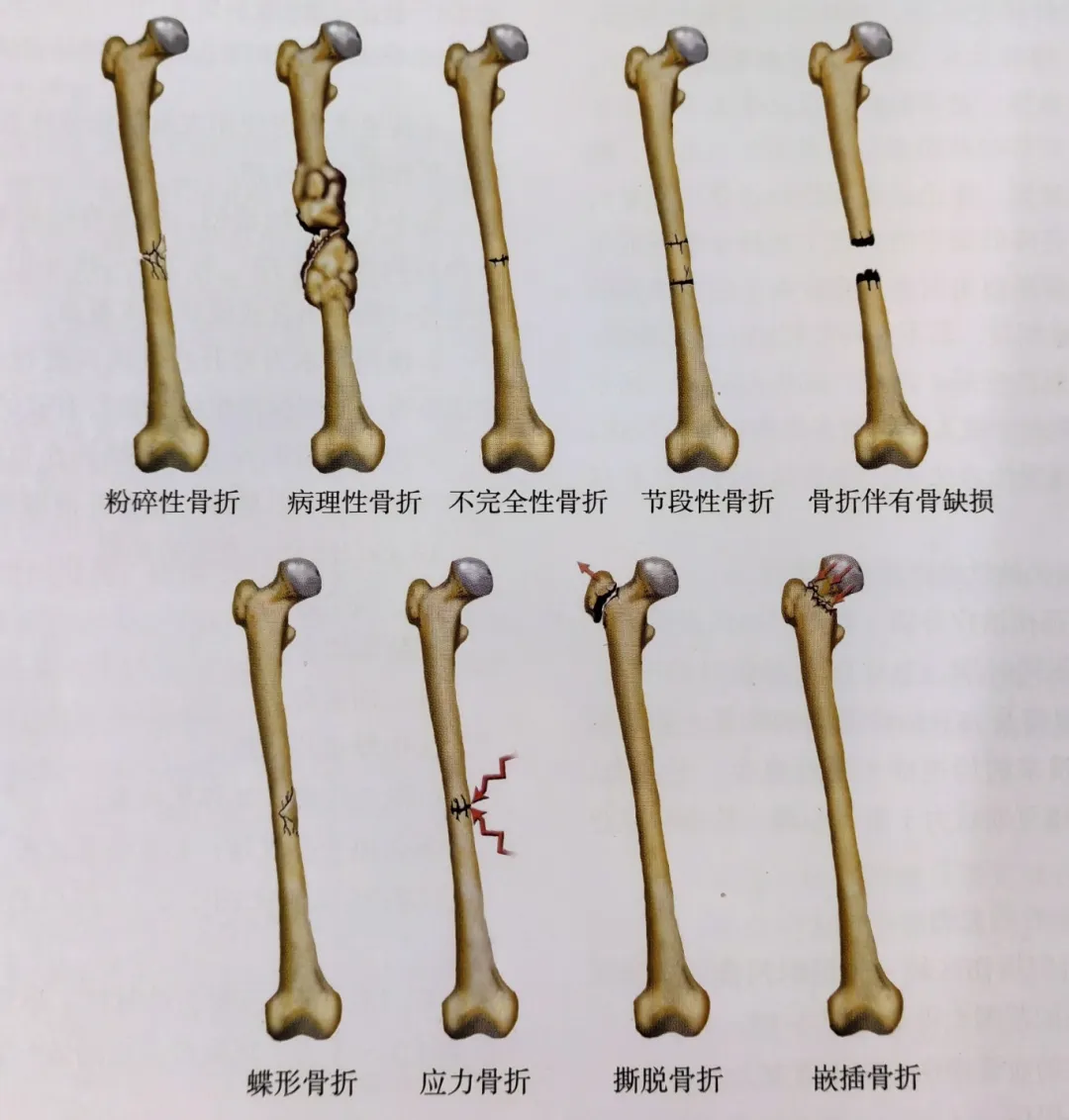
Figure 4: Classification of fractures
III.Factors influencing fracture healing
Biological factors: age, metabolic bone disease, underlying disease, functional level, nutritional status, neurological function, vascular damage, hormones, growth factors, health status of soft tissue capsule, degree of sterility (open fracture), smoking, medication, local pathology, traumatic energy level, type of bone, degree of bone defect, mechanical factors, degree of attachment of soft tissue to bone, stability, anatomical structure, level of traumatic energy, degree of bone defect.
IV. Modalities of treatment
Non-surgical treatment is indicated for patients with low-energy injuries or who are inoperable due to systemic or local factors.
Reducing: traction along the long axis of the limb, fracture separation.
Brace fixation at both ends of the fracture again: fixation of the reduced bone through external fixation, including three-point fixation technique.
Tubular bone continuous compression fixation technique traction: a way of reduction, including skin traction, bone traction.
Surgical treatment
(1) External fixation is suitable for open fractures, closed fractures with severe soft tissue trauma, and fractures accompanied by infection (Fig. 5)
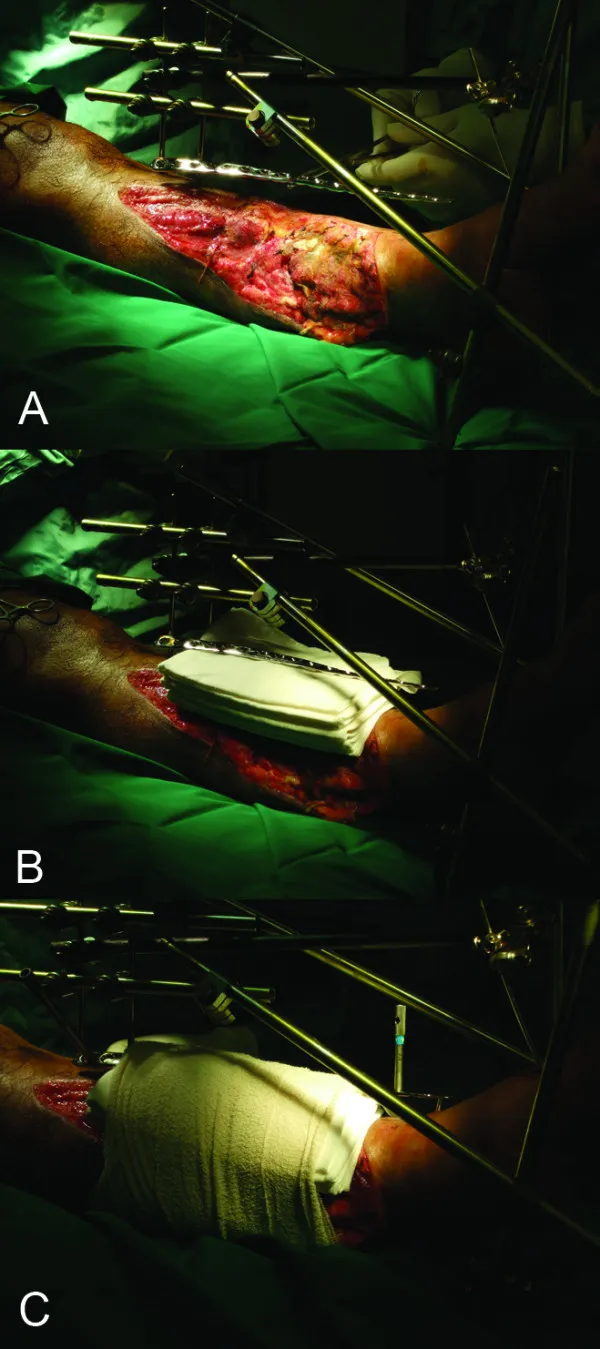
Figure 5: External fixation procedure
(2) Internal fixation is applicable to other types of fractures and follows the AO principle (Table 1)
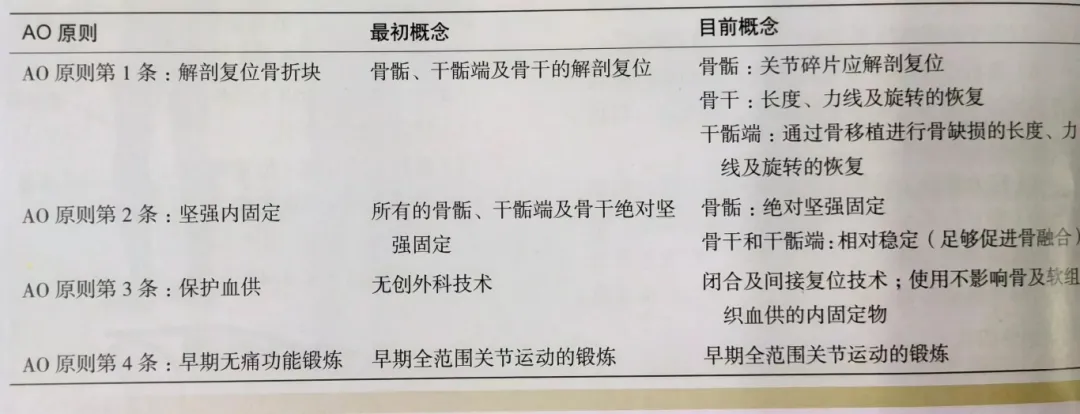
Table 1: Evolution of AO in fracture therapy
Interfracture fragments require compression fixation, including static compression (compression screws), dynamic compression (non-locking intramedullary nails), splinting (sliding between the internal object and bone), and bridging fixation (internal material spanning the comminuted area)
(4)Indirect reduction:
The traction technology is implemented in the fracture comminuted area to reduce the fragment through the tension of the soft tissue, and the traction force is derived from the femoral traction device, external fixator, AO joint tension device or lamina opener.
V.Staging of treatment
According to the biochemical process of fracture healing, it is divided into four stages (Table 2). At the same time, combined with the biochemical process, the treatment of fracture is divided into three stages, which promotes the completion of the biochemical process and the healing of the fracture (Fig. 6).
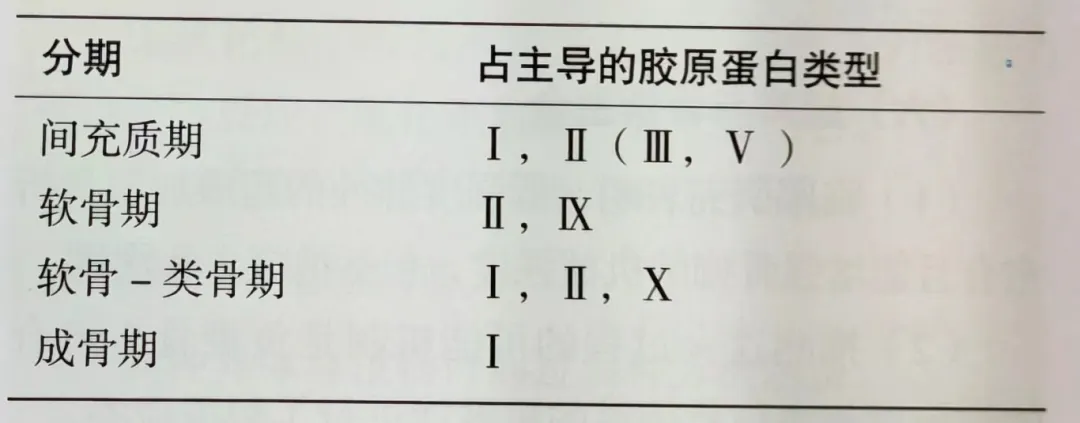
Table 2: Life course of fracture healing
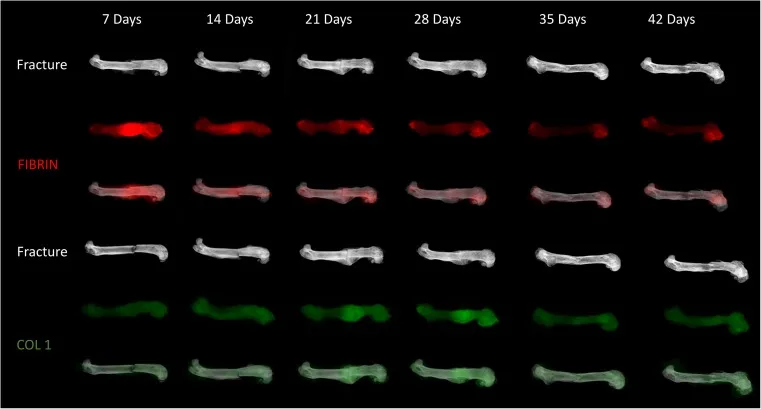
Figure 6: Schematic diagram of fracture healing in mice
Inflammatory phase
Hemorrhage from the fracture site and surrounding soft tissues forms a hematoma, fibrovascular tissue forms at the fractured end, and osteoblasts and fibroblasts begin to proliferate.
Downtime
The original callus response occurs within 2 weeks, with the formation of a cartilage skeleton followed by the formation of a callus through endochondral ossification, and all specific forms of fracture healing are related to the treatment modality.
Restruction
During the repair process, the braided bone formed is replaced by lamellar bone, and the medullary cavity is recanalized to mark the completion of fracture repair.
Complication
Delayed union is mainly manifested by the fracture not healing within the expected time frame, but still has some biological activity, and the reasons for delayed union are varied, which are related to the factors affecting fracture healing.
Nonunion is manifested as fracture without evidence of clinical or radiological healing, and the main realizations are:
(1)Atrophic nonunion due to nonvascularization and lack of biological ability to heal, typically manifested as stenosis of the broken end of the bone and no blood vessels, and the treatment process requires stimulation of local biological activity (bone graft or bone cortical resection and bone transport).
(2)Hypertrophic nonunion has transitional vascularization and biological ability, but lacks mechanical stability, which is typically manifested as overgrowth of the broken end of the fracture, and the treatment needs to increase mechanical stability (bone plate and screw fixation).
(3)The dystrophic nonunion has sufficient blood supply, but there is almost no callus formation, and the fracture reduction needs to be re-performed due to insufficient displacement and reduction of the broken end of the fracture.
(4)For infectious nonunion with chronic infection, the treatment should first remove the infection focus, and then promote fracture healing. Bone infection osteomyelitis is a disease of bone and bone infection, which can be direct infection of open wound wounds or pathogenic infection through bloodborne routes, and it is necessary to identify the infected microorganisms and pathogens before treatment.
Complex regional pain syndrome is characterized by pain, hyperesthesia, limb allergies, irregular local blood flow, sweating, and edema, including abnormalities of the autonomic nervous system. It usually occurs after trauma and surgery, and is detected and treated early, with sympathetic nerve block if necessary.
• Heterotopic ossification (HO) is common after trauma or surgery, and is more common in the elbow, hip, and thigh, and oral bisphosphonates can inhibit bone mineralization after symptomatic onset.
• Pressure in the periophysal compartment increases to a certain level, impairing internal perfusion.
• Neurovascular injury has different causes of neurovascular injury due to different anatomical locations.
• Avascular necrosis occurs in areas of insufficient blood supply, Specifically, see the injury and anatomical location, etc., and irreversible damage occurs.
Post time: Dec-31-2024





