




Surgical patient and site errors are serious and preventable. According to the Joint Commission on Accreditation of Healthcare Organizations, such errors can be made in up to 41% of orthopedic/pediatric surgeries. For spine surgery, a surgical site error occurs when a vertebral segment or lateralization is incorrect. In addition to failing to address the patient's symptoms and pathology, segmental errors can lead to new medical problems such as accelerated disc degeneration or spinal instability in otherwise asymptomatic or normal segments.
There are also legal issues associated with segmental errors in spine surgery, and the public, government agencies, hospitals, and societies of surgeons have zero tolerance for such errors. Many spinal surgeries, such as discectomy, fusion, laminectomy decompression, and kyphoplasty, are performed using a posterior approach, and proper positioning is important. Despite current imaging technology, segmental errors still occur, with incidence rates ranging from 0.032% to 15% reported in the literature. There is no conclusion as to which method of localization is most accurate.
Scholars from the Department of Orthopaedic Surgery at Mount Sinai School of Medicine, USA, conducted an online questionnaire study suggesting that the vast majority of spine surgeons use only a few methods of localization, and that clarification of the usual causes of error can be effective in reducing surgical segmental errors, in an article published May 2014 in Spine J. The study was conducted using an emailed questionnaire. The study was conducted using an emailed link to a questionnaire sent to members of the North American Spine Society (including orthopedic surgeons and neurosurgeons). The questionnaire was sent only once, as recommended by the North American Spine Society. A total of 2338 physicians received it, 532 opened the link, and 173 (7.4% response rate) completed the questionnaire. Seventy-two percent of the completers were orthopedic surgeons, 28% were neurosurgeons, and 73% were spine physicians in training.
The questionnaire consisted of a total of 8 questions (Fig. 1) covering the most commonly used methods of localization (both anatomical landmarks and imaging localization), the incidence of surgical segmental errors, and the association between methods of localization and segmental errors. The questionnaire was not pilot tested or validated. The questionnaire allows for multiple answer choices.
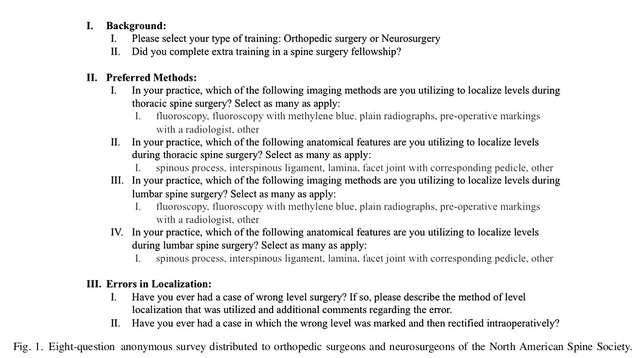
Figure 1 Eight questions from the questionnaire. The results showed that intraoperative fluoroscopy was the most commonly used method of localization for posterior thoracic and lumbar spine surgery (89% and 86%, respectively), followed by radiographs (54% and 58%, respectively). 76 physicians chose to use a combination of both methods for localization. The spinous processes and corresponding pedicles were the most commonly used anatomic landmarks for thoracic and lumbar spine surgery (67% and 59%), followed by the spinous processes (49% and 52%) (Fig. 2). 68% of physicians admitted that they had made segmental localization errors in their practice, some of which were corrected intraoperatively (Fig. 3).
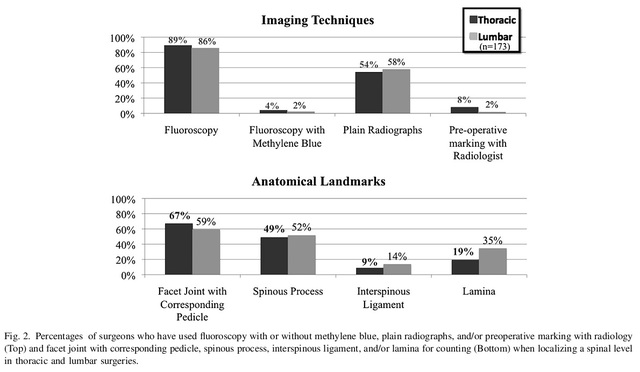
Fig. 2 Imaging and anatomical landmark localization methods used.
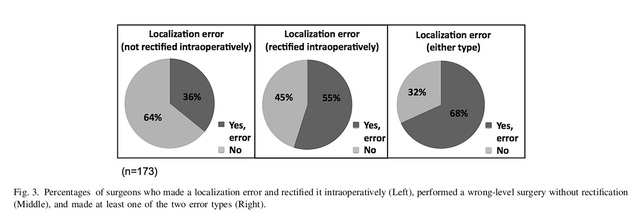
Fig. 3 Physician and intraoperative correction of surgical segment errors.
For localization errors, 56% of these physicians used preoperative radiographs and 44% used intraoperative fluoroscopy. The usual reasons for preoperative positioning errors were failure to visualize a known reference point (e.g., the sacral spine was not included in the MRI), anatomical variations (lumbar displaced vertebrae or 13-root ribs), and segmental ambiguities due to the patient's physical condition (suboptimal X-ray display). Common causes of intraoperative positioning errors include inadequate communication with the fluoroscopist, failure of repositioning after positioning (movement of the positioning needle after fluoroscopy), and incorrect reference points during positioning (lumbar 3/4 from the ribs down) (Figure 4).
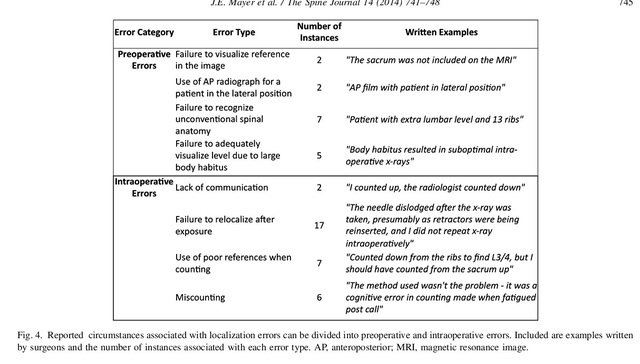
Fig. 4 Reasons for preoperative and intraoperative localization errors.
The above results show that although there are many methods of localization, the vast majority of surgeons use only a few of them. Although surgical segmental errors are rare, ideally they are absent. There is no standard way to eliminate these errors; however, taking the time to perform positioning and identifying the usual causes of positioning errors can help reduce the incidence of surgical segmental errors in the thoracolumbar spine.
Post time: Jul-24-2024





