




Ankle fractures are one of the most common types of fractures in clinical practice. Except for some Grade I/II rotational injuries and abduction injuries, most ankle fractures usually involve the lateral malleolus. Weber A/B type lateral malleolus fractures typically result in stable distal tibiofibular syndesmosis and can achieve good reduction with direct visualization from distal to proximal. In contrast, C-type lateral malleolus fractures involve instability in the lateral malleolus across three axes due to distal tibiofibular injury, which can lead to six types of displacement: shortening/lengthening, widening/narrowing of the distal tibiofibular space, anterior/posterior displacement in the sagittal plane, medial/lateral tilt in the coronal plane, rotational displacement, and combinations of these five types of injuries.
Numerous previous studies have shown that shortening/lengthening can be assessed through evaluating the Dime sign, Stenton line, and tibial-gapping angle, among others. Displacement in the coronal and sagittal planes can be well-assessed using frontal and lateral fluoroscopic views; however, rotational displacement is the most challenging to assess intraoperatively.
The difficulty in assessing rotational displacement is particularly evident in the reduction of the fibula when inserting the distal tibiofibular screw. Most literature indicates that after the insertion of the distal tibiofibular screw, there is a 25%-50% occurrence of poor reduction, resulting in the malunion and fixation of fibular deformities. Some scholars have proposed using routine intraoperative CT assessments, but this can be challenging to implement in practice. To address this issue, in 2019, Professor Zhang Shimin's team from Yangpu Hospital affiliated with Tongji University published an article in the international orthopedic journal *Injury*, proposing a technique for assessing whether the lateral malleolus rotation has been corrected using intraoperative X-ray. The literature reports significant clinical efficacy of this method.
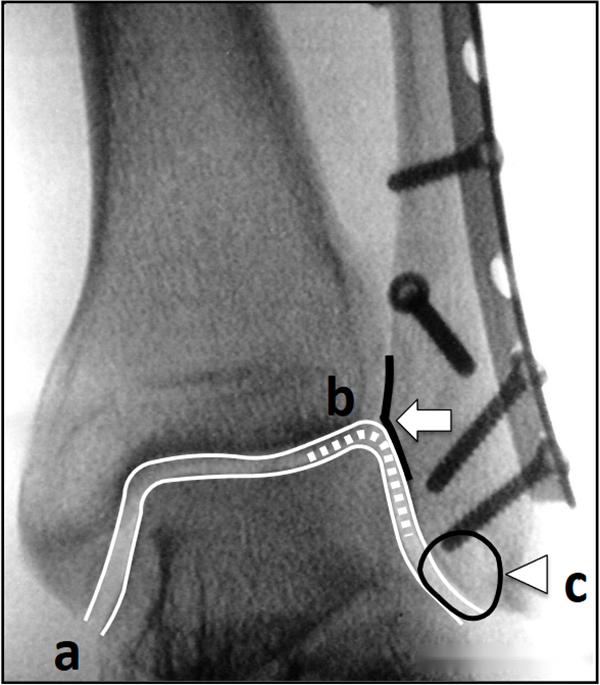
The theoretical basis of this method is that in the fluoroscopic view of the ankle, the lateral wall cortex of the lateral malleolar fossa shows a clear, vertical, dense shadow, parallel to the medial and lateral cortices of the lateral malleolus, and located at the middle to outer one-third of the line connecting the medial and lateral cortices of the lateral malleolus.
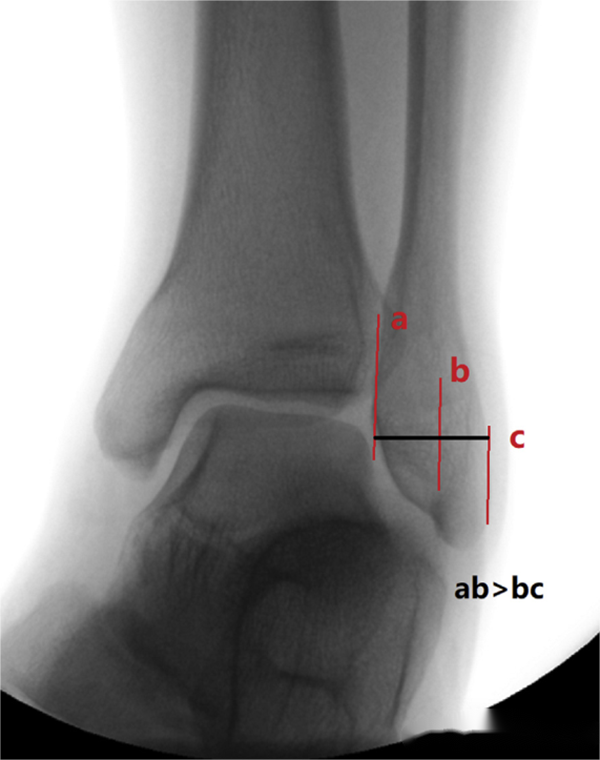
Illustration of the ankle fluoroscopic view showing the positional relationship between the lateral wall cortex of the lateral malleolar fossa (b-line) and the medial and lateral cortices of the lateral malleolus (a and c lines). Typically, the b-line is located on the outer one-third line between lines a and c.
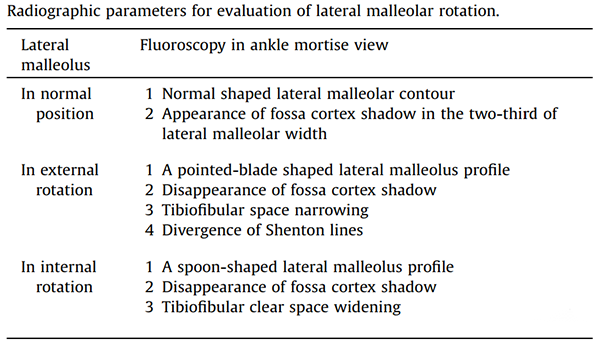
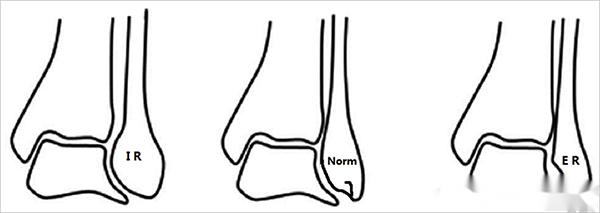
The normal position of the lateral malleolus, external rotation, and internal rotation can produce different imaging appearances in the fluoroscopic view:
- Lateral malleolus rotated in a normal position**: A normal lateral malleolus contour with a cortical shadow on the lateral wall of the lateral malleolar fossa, positioned on the outer one-third line of the medial and lateral cortices of the lateral malleolus.
-Lateral malleolus external rotation deformity**: The lateral malleolus contour appears "sharp-leafed," the cortical shadow on the lateral malleolar fossa disappears, the distal tibiofibular space narrows, the Shenton line becomes discontinuous and dispersed.
-Lateral malleolus internal rotation deformity**: The lateral malleolus contour appears "spoon-shaped," the cortical shadow on the lateral malleolar fossa disappears, and the distal tibiofibular space widens.
The team included 56 patients with C-type lateral malleolar fractures combined with distal tibiofibular syndesmosis injuries and used the aforementioned evaluation method. Postoperative CT re-examinations showed that 44 patients achieved anatomic reduction with no rotational deformities, while 12 patients experienced mild rotational deformity (less than 5°), with 7 cases of internal rotation and 5 cases of external rotation. No cases of moderate (5-10°) or severe (greater than 10°) external rotation deformities occurred.
Previous studies have indicated that the assessment of lateral malleolar fracture reduction can be based on the three main Weber parameters: parallel equidistance between the tibial and talar joint surfaces, continuity of the Shenton line, and the Dime sign.
Poor reduction of the lateral malleolus is a very common issue in clinical practice. While proper attention is given to the restoration of length, equal importance should be placed on the correction of rotation. As a weight-bearing joint, any malreduction of the ankle can have catastrophic effects on its function. It is believed that the intraoperative fluoroscopic technique proposed by Professor Zhang Shimin can assist in achieving precise reduction of C-type lateral malleolar fractures. This technique serves as a valuable reference for frontline clinicians.
Post time: May-06-2024





