




The conventional lateral L approach is the classic approach for the surgical treatment of calcaneal fractures. Although the exposure is thorough, the incision is long and the soft tissue is stripped more, which easily leads to complications such as delayed soft tissue union, necrosis, and infection. Coupled with the current society’s pursuit of minimally invasive aesthetics, minimally invasive surgical treatment of calcaneal fractures has been highly praised. This article has compiled 8 tips.
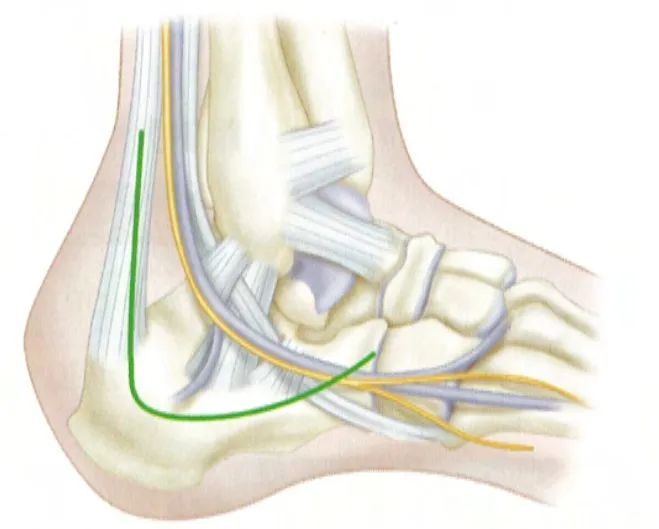
With a wide lateral approach, the vertical part of the incision starts slightly proximal to the tip of the fibula and anterior to the Achilles tendon. The level of the incision is made just distal to the bruised skin fed by the lateral calcaneal artery and inserts at the base of the fifth metatarsal. The two parts are connected at the heel to form a slightly curved right angle. Source: Campbell Orthopedic Surgery.
Percutaneous poking reduction
In the 1920s, Böhler developed the minimally invasive treatment method of reduction of the calcaneus under traction, and for a long time thereafter, percutaneous poking reduction under traction became the mainstream method for the treatment of calcaneus fractures.
It is suitable for fractures with less displacement of intraarticular fragments in the subtalar joint, such as Sanders type II and some Sanders III lingual fractures.
For Sanders type III and comminuted Sanders type IV fractures with severe subtalar articular surface collapse, poking reduction is difficult and it is difficult to achieve anatomical reduction of the posterior articular surface of the calcaneus.
It is difficult to restore the width of the calcaneus, and the deformity cannot be well corrected. It often leaves the lateral wall of the calcaneus in varying degrees, resulting in the impact of the lower lateral malleolus with the lateral wall of the calcaneus, displacement or compression of the peroneus longus tendon, and impingement of the peroneal tendon. Syndrome, calcaneal impingement pain, and peroneus longus tendonitis.
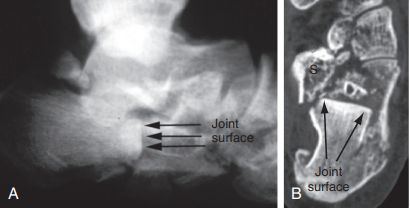
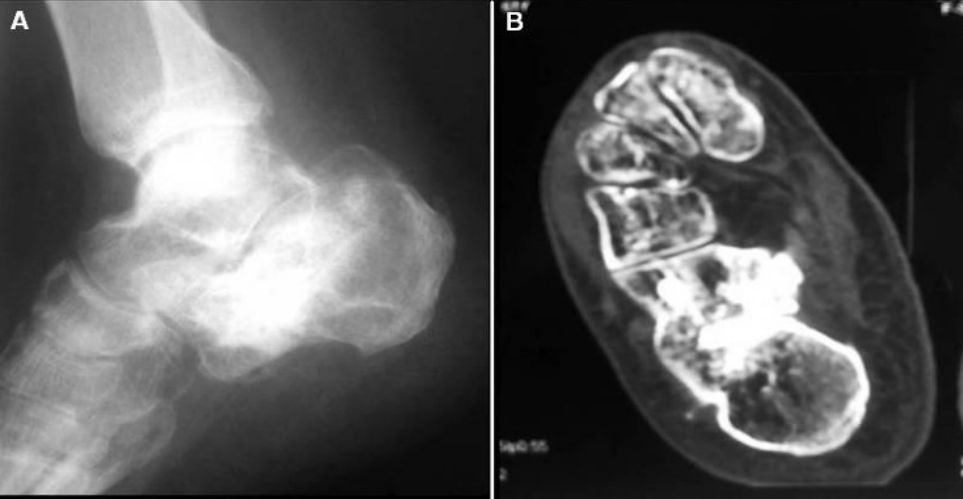
Westhues/Essex-lopresti technique. A. Lateral fluoroscopy confirmed the collapsed tongue-shaped fragment; B. A horizontal plane CT scan showed a Sandess type IIC fracture. The anterior portion of the calcaneus is clearly comminuted in both images. S. Carrying distance sudden.
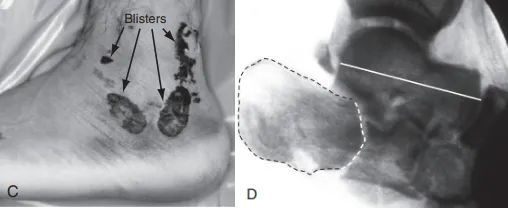
C. Lateral incision could not be used because of severe soft tissue swelling and blistering; D. Lateral fluoroscopy showing articular surface (dotted line) and talar collapse (solid line).
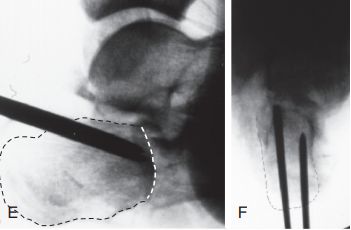
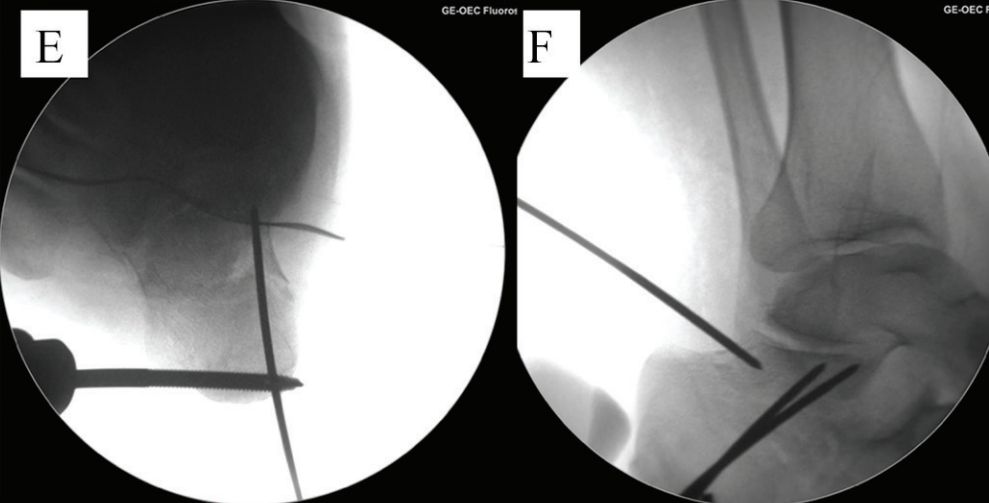
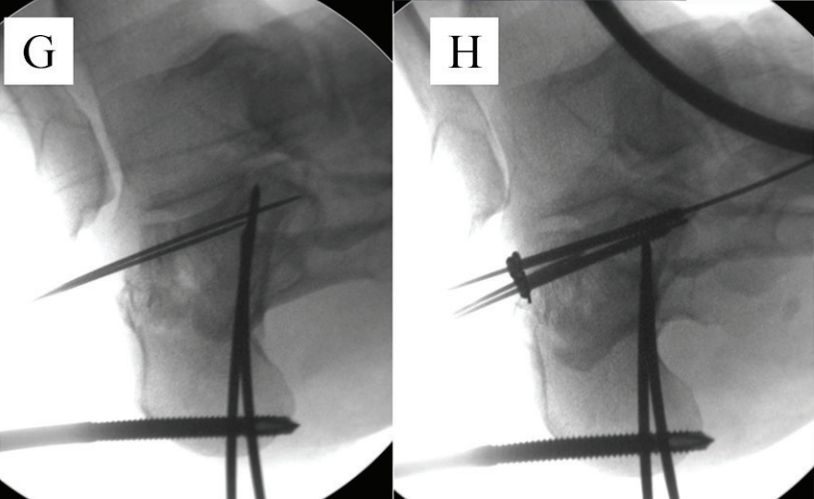
E and F. Two hollow nail guide wires were placed parallel to the lower part of the tongue-shaped fragment, and the dotted line is the joint line.
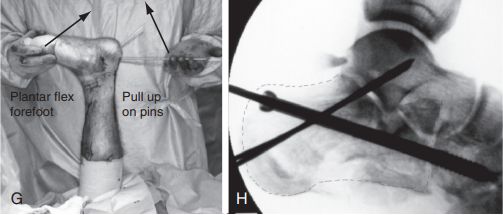
G. Flex the knee joint, pry up the guide pin, and at the same time plantar flex the midfoot to reduce the fracture: H. One 6.5 mm cannulated screw was fixed to the cuboid bone and two 2.0 mm Kirschner wires were subspan articulated to maintain reduction due to calcaneus anterior comminution. Source: Mann Foot and Ankle Surgery.
Sinus tarsi incision
The incision is made 1 cm distal to the tip of the fibula to the base of the fourth metatarsal. In 1948, Palmer first reported a small incision in the sinus tarsi.
In 2000, Ebmheim et al. used the tarsal sinus approach in the clinical treatment of calcaneal fractures.
o Can fully expose the subtalar joint, posterior articular surface and anterolateral fracture block;
o Adequately avoid the lateral calcaneal blood vessels;
o There is no need to cut the calcaneofibular ligament and subperoneal retinaculum, and the joint space can be increased by proper inversion during the operation, which has the advantages of small incision and less bleeding.
The disadvantage is that the exposure is obviously insufficient, which limits and affects the fracture reduction and the placement of internal fixation. It is only suitable for Sanders type I and type II calcaneal fractures.

Oblique small incision
A modification of the sinus tarsi incision, approximately 4 cm in length, centered 2 cm below the lateral malleolus and parallel to the posterior articular surface.
If the preoperative preparation is sufficient and conditions permit, it can also have a good reduction and fixation effect on Sanders type II and III intra-articular calcaneal fractures; if subtalar joint fusion is required in the long term, the same incision can be used.
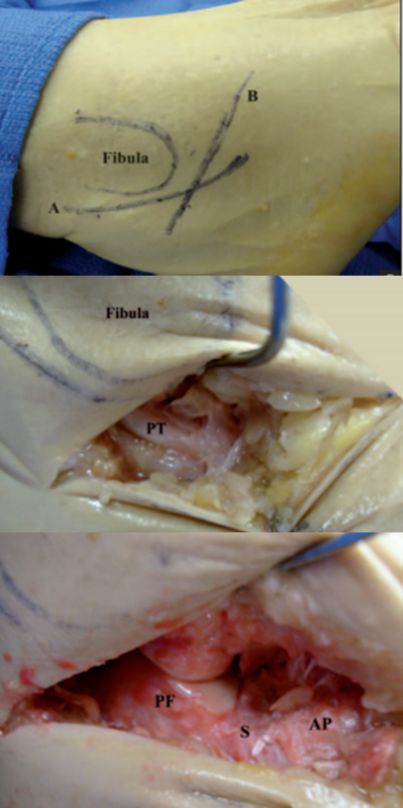
PT Peroneal tendon. PF Posterior articular surface of the calcaneus. S sinus tarsi. AP Calcaneal protrusion. .
Posterior longitudinal incision
Starting from the midpoint of the line between the Achilles tendon and the tip of the lateral malleolus, it extends vertically down to the talar heel joint, with a length of about 3.5 cm.
Less incision is made in the far soft tissue, without damaging important structures, and the posterior articular surface is well exposed. After percutaneous prying and reduction, an anatomical board was inserted under the guidance of intraoperative perspective, and the percutaneous screw was tapped and fixed under pressure.
This method can be used for Sanders type I, II, and III, especially for displaced posterior articular surface or tuberosity fractures.

Herringbone cut
Modification of sinus tarsi incision. From 3 cm above the tip of the lateral malleolus, along the posterior border of the fibula to the tip of the lateral malleolus, and then to the base of the fourth metatarsal. It allows good reduction and fixation of Sanders type II and III calcaneal fractures, and can be extended if necessary to expose the transfibula, talus, or lateral column of the foot.
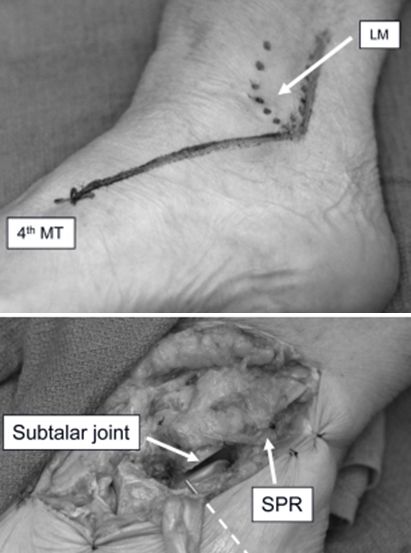
LM lateral ankle. MT metatarsal joint. SPR Supra fibula retinaculum.
Arthroscopically assisted reduction
In 1997, Rammelt proposed that subtalar arthroscopy can be used to reduce the posterior articular surface of the calcaneus under direct vision. In 2002, Rammelt first performed arthroscopically assisted percutaneous reduction and screw fixation for Sanders type I and II fractures.
Subtalar arthroscopy mainly plays a monitoring and auxiliary role. It can observe the condition of the subtalar articular surface under direct vision, and assist in monitoring the reduction and internal fixation. Simple subtalar joint dissection and osteophyte resection can also be performed.
The indications are narrow: only for Sanders type Ⅱ with mild comminution of the articular surface and AO/OTA type 83-C2 fractures; while for Sanders Ⅲ, Ⅳ and AO/OTA type 83-C3 Fractures with articular surface collapse such as 83-C4 and 83-C4 are more difficult to operate.

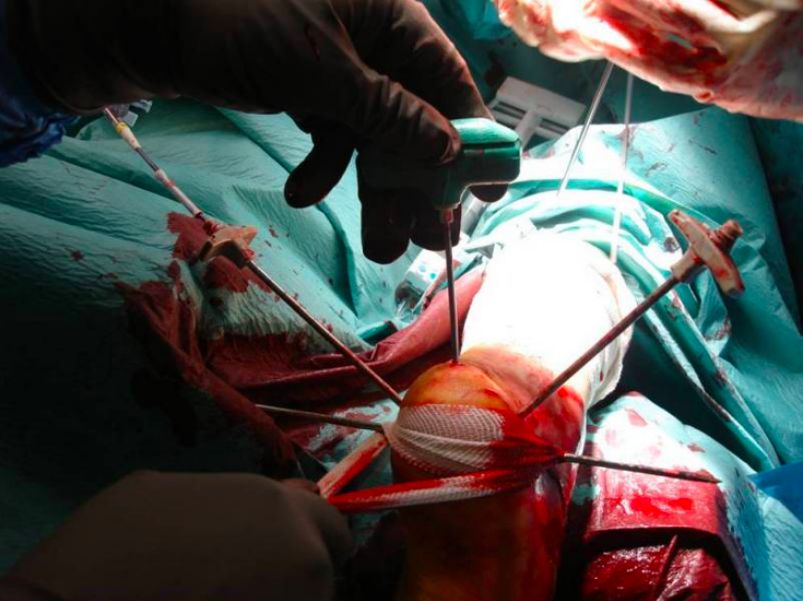
body position
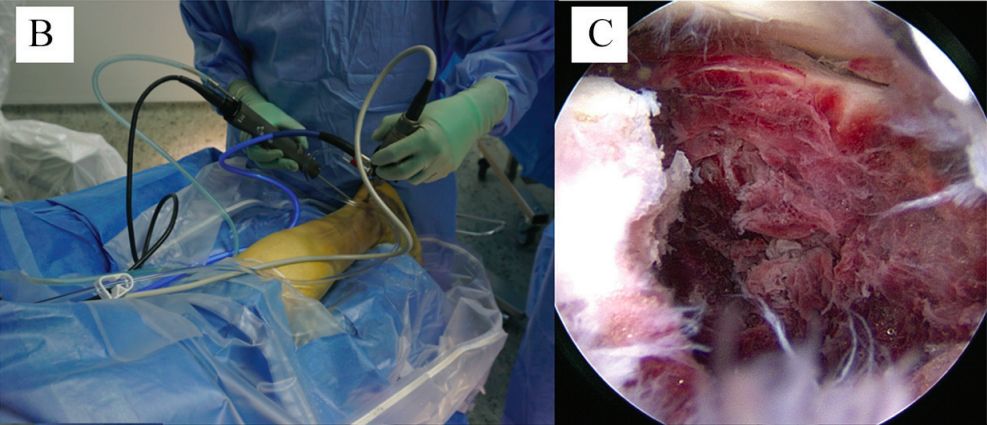
b. Posterior ankle arthroscopy. c. Access to the fracture and subtalar joint.

Schantz screws were placed.
e. Reset and temporary fixation. f. After reset.
g. Temporarily fix the articular surface bone block. h. Fix with screws.
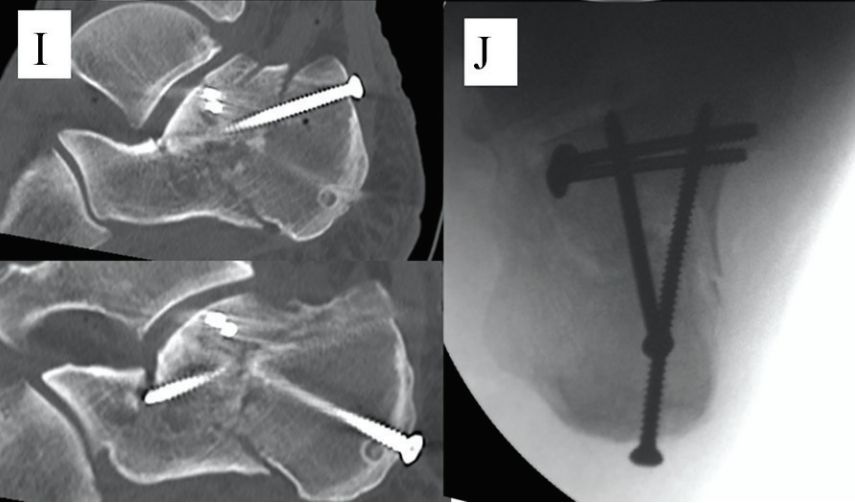
i. Postoperative sagittal CT scan. j. Postoperative axial perspective.
In addition, the subtalar joint space is narrow, and traction or brackets are needed to support the joint space to facilitate the placement of the arthroscope; the space for intra-articular manipulation is small, and careless manipulation can easily cause iatrogenic cartilage surface damage; unskilled surgical techniques are prone to local injury organize.
Percutaneous balloon angioplasty
In 2009, Bano first proposed the balloon dilatation technique for the treatment of calcaneal fractures. For Sanders type II fractures, most of the literature considers the effect to be definite. But other types of fractures are more difficult.
Once the bone cement infiltrates into the subtalar joint space during the operation, it will cause the wear of the articular surface and the limitation of joint motion, and the balloon expansion will not be balanced for fracture reduction.
Placement of cannula and guide wire under fluoroscopy
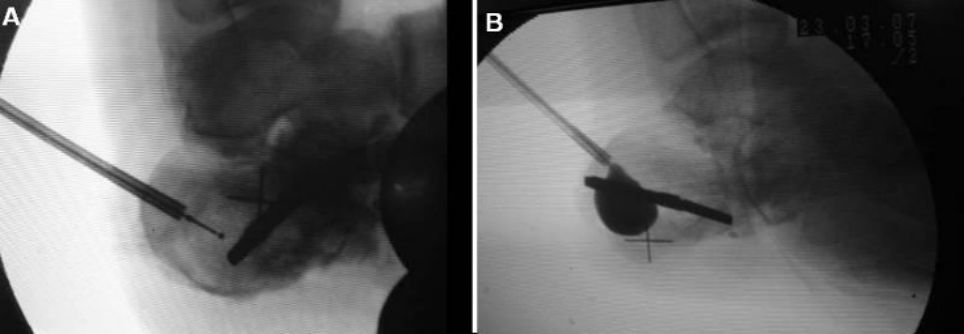
Images before and after airbag inflation
X-ray and CT images two years after surgery.
At present, the research samples of balloon technology are generally small, and most of the fractures with good results are caused by low-energy violence. Further research is still needed for calcaneal fractures with severe fracture displacement. It has been carried out for a short period of time, and the long-term efficacy and complications are still unclear.
Calcaneal intramedullary nail
In 2010, the calcaneal intramedullary nail came out. In 2012, M.Goldzak minimally invasive treatment of calcaneal fractures with intramedullary nailing. It should be emphasized that reduction cannot be achieved with intramedullary nailing.
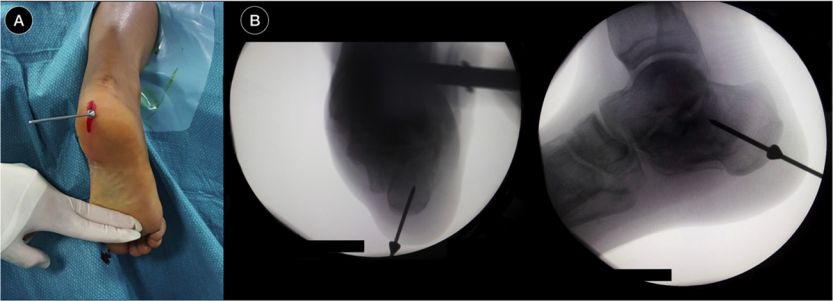
Insert positioning guide pin, fluoroscopy
Repositioning the subtalar joint
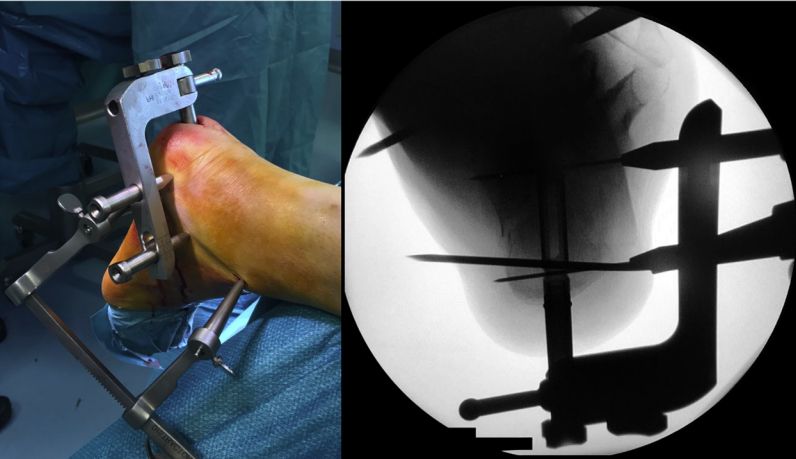
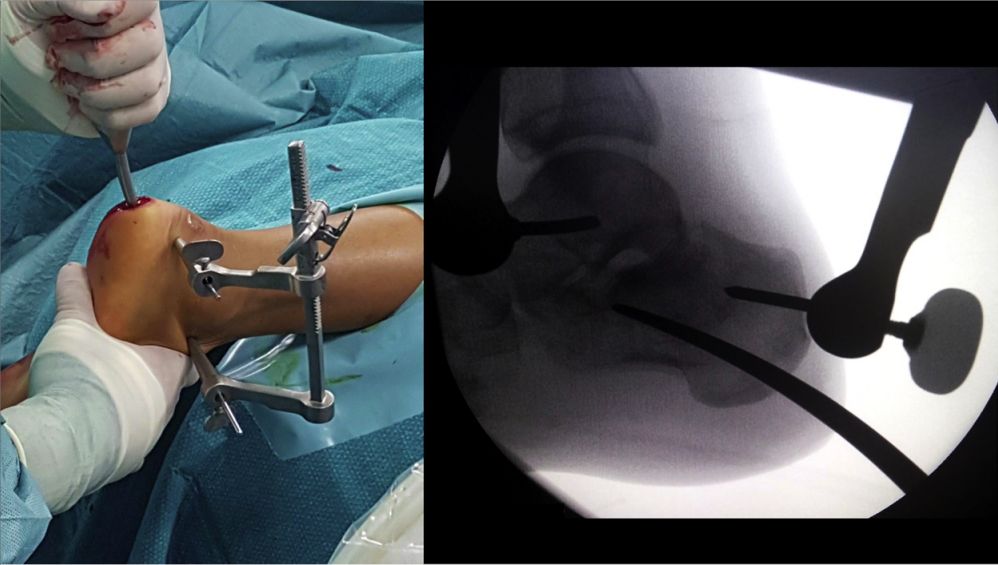
Place the positioning frame, drive the intramedullary nail, and fix it with two 5 mm cannulated screws
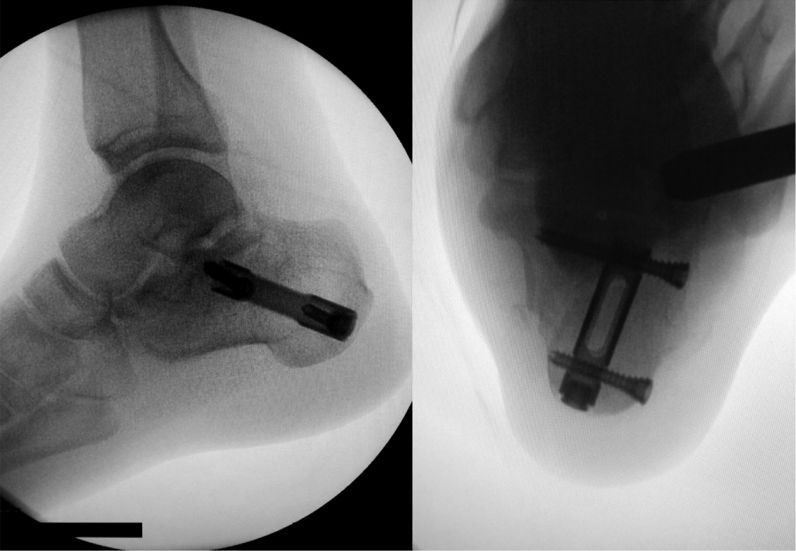
Perspective after intramedullary nail placement.
Intramedullary nailing has been shown to be successful in the treatment of Sanders type II and III fractures of the calcaneus. Although some physicians tried to apply it to Sanders IV fractures, the reduction operation was difficult and ideal reduction could not be obtained.
Contact Person: Yoyo
WA/TEL:+8615682071283
Post time: May-31-2023





