




Transverse fracture with slight or no comminution: in the case of a fracture of the metacarpal bone (neck or diaphysis), reset by manual traction. The proximal phalanx is maximally flexed to expose the head of the metacarpal. A 0.5- 1 cm transverse incision is made and the extensor tendon is retracted longitudinally in the midline. Under fluoroscopic guidance, we inserted a 1.0 mm guide wire along the longitudinal axis of the wrist. The tip of the guidewire was blunted in order to avoid cortical penetration and to facilitate sliding within the medullary canal. After the guidewire position was determined fluoroscopically, the subchondral bone plate was reamed using only a hollow drill bit. The appropriate screw length was calculated from preoperative images. In most metacarpal fractures, with the exception of the fifth metacarpal, we use a 3.0-mm diameter screw. We used AutoFIX headless hollow screws (little Bone Innovations, Morrisville, PA).The maximum usable length of a 3.0-mm screw is 40 mm. This is shorter than the average length of the metacarpal bone (approximately 6.0 cm), but long enough to engage the threads in the medulla to obtain secure fixation of the screw. The diameter of the medullary cavity of the fifth metacarpal is usually large, and here we used a 4.0 mm screw with a maximum diameter of up to 50 mm. At the end of the procedure, we ensure that the caudal thread is completely buried below the cartilage line. Conversely, it is important to avoid implanting the prosthesis too deeply, especially in the case of neck fractures.
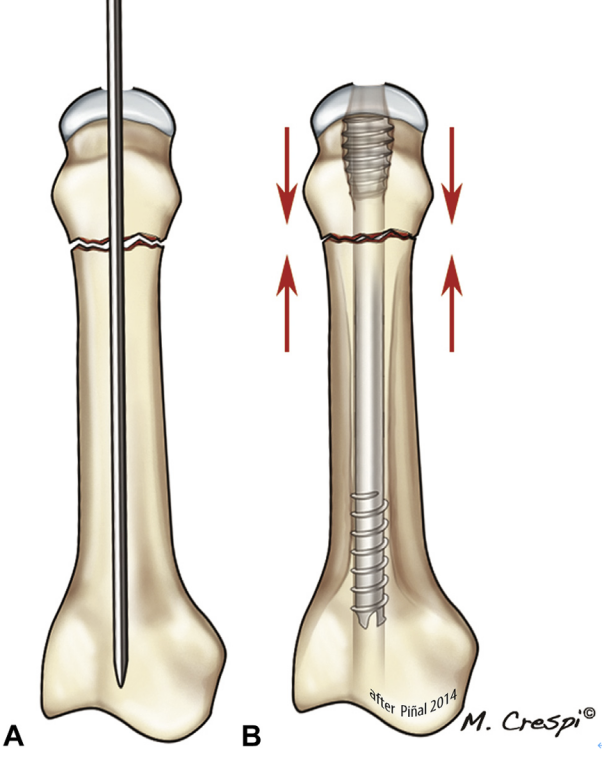
Fig. 14 In A, the typical neck fracture is not comminuted and the head requires minimal depth as the B cortex will be compressed
The surgical approach for a transverse fracture of the proximal phalanx was similar (Fig. 15). We made a 0.5 cm transverse incision at the head of the proximal phalanx while maximally flexing the proximal interphalangeal joint. The tendons were separated and retracted longitudinally to expose the head of the proximal phalanx. For most fractures of the proximal phalanx, we use a 2.5 mm screw, but for larger phalanges we use a 3.0 mm screw. The maximum length of the 2.5 mm CHS currently used is 30 mm. We take care not to over-tighten the screws. Since the screws are self-drilling and self-tapping, they may penetrate the base of the phalanx with minimal resistance. A similar technique was used for midphalangeal phalangeal fractures, with the incision starting at the head of the midphalangeal phalanx to allow retrograde placement of the screws.
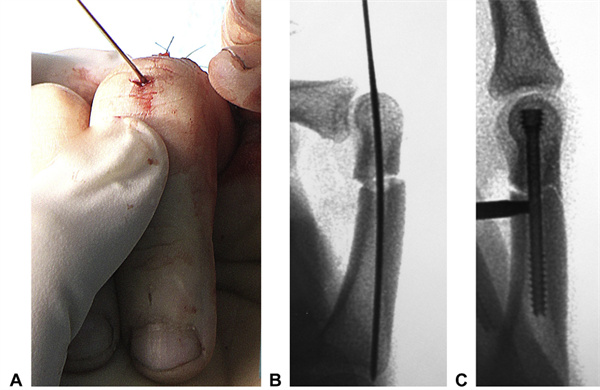
Fig. 15 Intraoperative view of a transverse phalanx case.A A 1-mm guidewire was placed through a small transverse incision along the longitudinal axis of the proximal phalanx.B The guidewire was placed to allow for fine-tuning of the repositioning and correction of any rotations.C A 2.5-mm CHS has been inserted and buried in the head. Due to the particular shape of the phalanges, compression may result in separation of the metacarpal cortex. (Same patient as in Figure 8)
Comminuted fractures: unsupported compression during insertion of the CHS can lead to shortening of the metacarpals and phalanges (Fig. 16). Therefore, despite the fact that the use of the CHS is in principle prohibited in such cases, we have found a solution to the two most common scenarios we face.
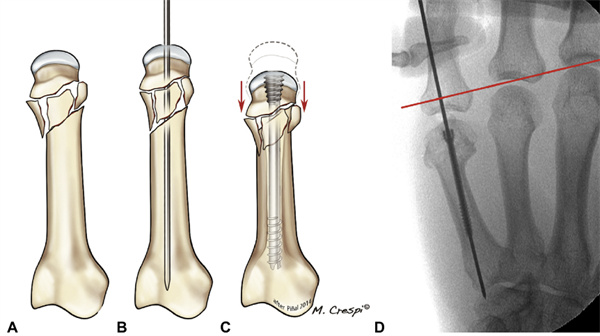
FIGURE 16 A-C If the fracture is not cortically supported, tightening the screws will result in fracture collapse despite complete reduction.D Typical examples from the authors' series corresponding to cases of maximum shortening (5 mm). The red line corresponds to the metacarpal line.
For submetacarpal fractures, we use a modified technique based on the architectural concept of bracing (i.e., structural elements used to support or reinforce a frame by resisting longitudinal compression and thus supporting it). By forming a Y-shape with two screws, the head of the metacarpal does not collapse; we named this the Y-shape brace. As in the previous method, a 1.0 mm longitudinal guide wire with a blunt tip is inserted. While maintaining the correct length of the metacarpal, another guide wire is inserted, but at an angle to the first guide wire, thus forming a triangular structure. Both guidewires were expanded using a guided countersink to expand the medulla. For axial and oblique screws, we usually use 3.0 mm and 2.5 mm diameter screws, respectively. The axial screw is first inserted until the caudal thread is level with the cartilage. An offset screw of appropriate length is then inserted. Since there is not enough room in the medullary canal for two screws, the length of the oblique screws needs to be carefully calculated, and the axial screws should only be attached to the axial screws once they are sufficiently buried in the metacarpal head to ensure adequate stability without screw protrusion. The first screw is then advanced forward until it is fully buried. This avoids axial shortening of the metacarpal and collapse of the head, which can be prevented by oblique screws. We perform frequent fluoroscopic examinations to ensure that collapse does not occur and that the screws are interlocked within the medullary canal (Fig. 17).
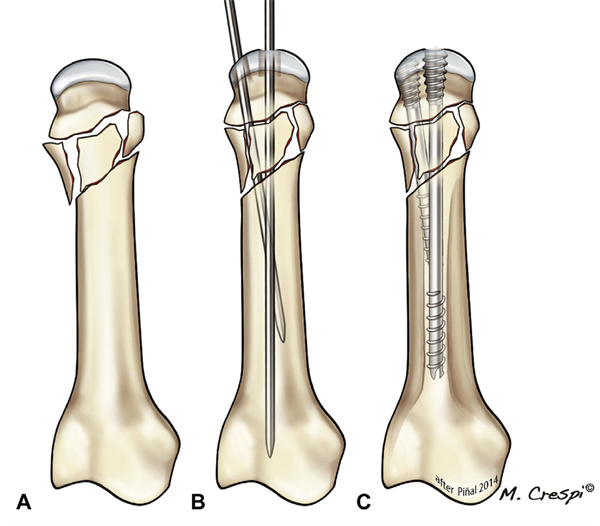
Figure 17 A-C Y-bracket technology
When comminution affected the dorsal cortex at the base of the proximal phalanx, we devised a modified method; we named it axial bracing because the screw acts as a beam within the phalanx. After resetting the proximal phalanx, the axial guide wire was introduced into the medullary canal as dorsally as possible. A CHS slightly shorter than the total length of the phalanx (2.5 or 3.0 mm) is then inserted until its anterior end meets the subchondral plate at the base of the phalanx. At this point, the caudal threads of the screw are locked into the medullary canal, thus acting as an internal support and bracing the base of the phalanx. Multiple fluoroscopic examinations are required to prevent joint penetration (Figure 18). Depending on the fracture pattern, other screws or combinations of internal fixation devices may be required (Figure 19).
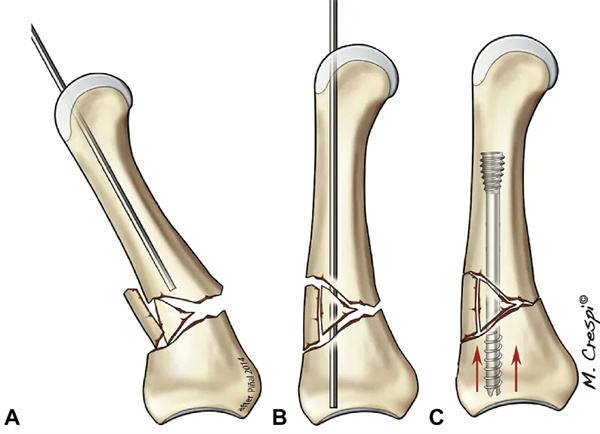

Figure 19: Different methods of fixation in patients with crush injuries. Severe comminuted submetacarpal fracture of the ring finger with compound dislocation of the base of the middle finger (yellow arrow pointing to the area of the comminuted fracture).B Standard 3.0 mm CHS of the index finger was used, 3.0 mm paracentesis of the comminuted middle finger, y-support of the ring finger (and one-stage grafting of the defect), and 4.0 mm CHS of the pinky finger.F Free flaps were used for soft-tissue coverage.C Radiographs at 4 months. The metacarpal bone of the little finger healed. Some bone scabs formed elsewhere, indicating secondary fracture healing.D One year after the accident, the flap was removed; although asymptomatic, a screw was removed from the metacarpal of the ring finger because of suspected intra-articular penetration. Good results (≥240° TAM) were obtained in each finger at the last visit.Changes in the metacarpophalangeal joint of the middle finger were evident at 18 months.
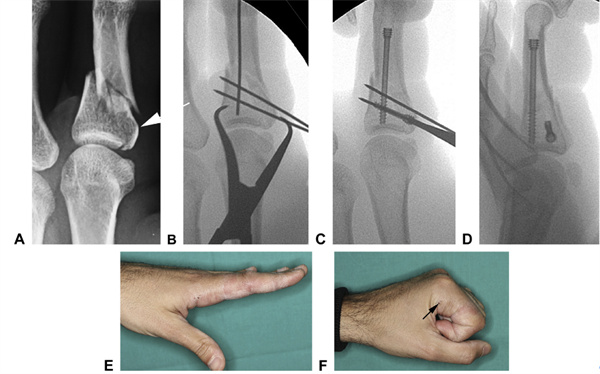
Fig. 20 A Fracture of the index finger with intra-articular extension (shown by arrows), which was converted to a simpler fracture by B temporary fixation of the articular fracture using a K-wire.C This created a stable base in which a supporting longitudinal screw was inserted.D After fixation, the construct was judged to be stable, permitting immediate active movement.E,F Range of motion at 3 weeks (arrows marking the points of entry of the basal screws)
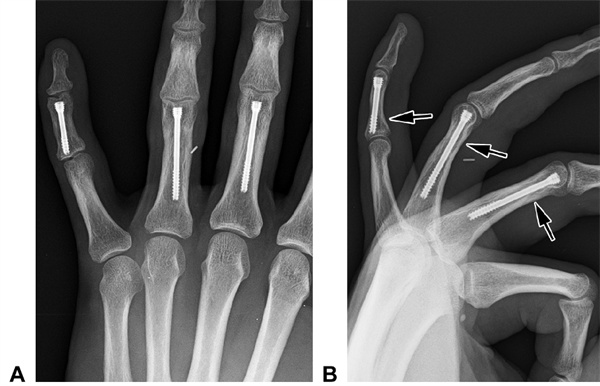
Fig. 21 Posterior orthostatic and B lateral radiographs of patient A. The patient's three transverse fractures (at the arrows) were treated with 2.5-mm cannulated screws. no significant changes in the interphalangeal joints were evident after 2 years
Post time: Sep-18-2024





