




Ankle injuries are a common sports injury that occurs in about 25% of musculoskeletal injuries, with lateral collateral ligament (LCL) injuries being the most common. If the severe condition is not treated in time, it is easy to lead to repeated sprains, and more serious cases will affect the function of the ankle joint. Therefore, it is of great significance to diagnose and treat patients' injuries at an early stage. This article will focus on the diagnostic skills of lateral collateral ligament injuries of the ankle joint to help clinicians improve the accuracy of diagnosis.
I. Anatomy
Anterior talofibular ligament (ATFL): flattened, fused to the lateral capsule, starting anterior to the fibula and ending anterior to the body of the talus.
Calcaneofibular ligament (CFL): cord-shaped, originating at the anterior border of the distal lateral malleolus and terminating at the calcaneus.
Posterior talofibular ligament (PTFL): Originates on the medial surface of the lateral malleolus and ends posterior to the medial talus.
ATFL alone accounted for about 80% of the injuries, while ATFL combined with CFL injuries accounted for about 20%.
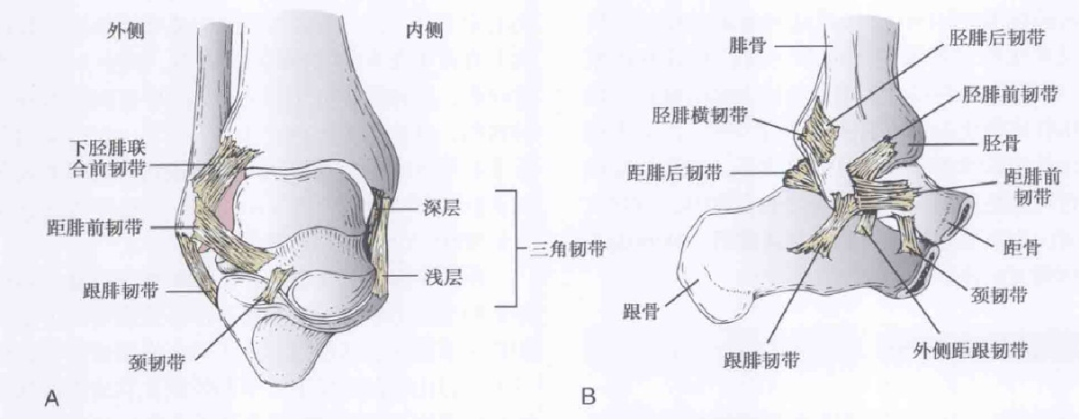
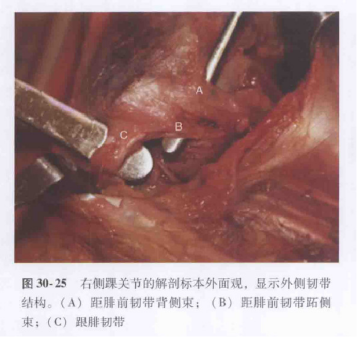
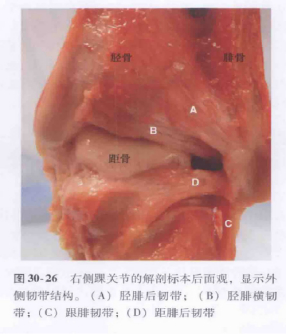
Schematic diagram and anatomical diagram of the lateral collateral ligament of the ankle joint
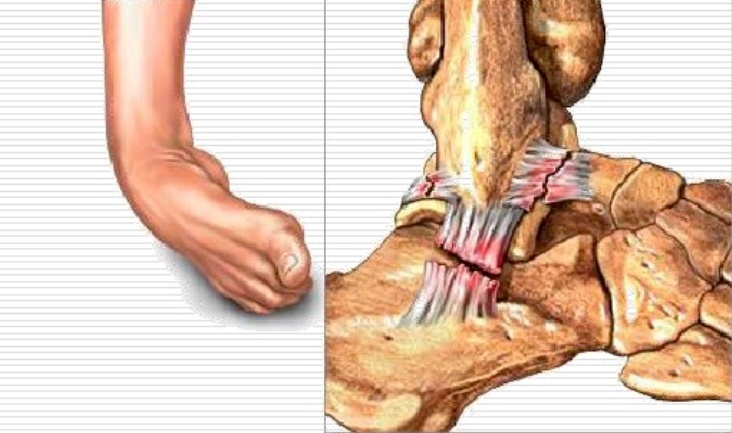
II. Mechanism of injury
Supinated injuries: anterior talofibular ligament
calcaneofibular ligament varus injury: calcaneofibular ligament
III. Injury grading
Grade I: ligament strain, no visible ligament rupture, rarely swelling or tenderness, and no signs of loss of function;
Grade II: partial macroscopic rupture of the ligament, moderate pain, swelling, and tenderness, and minor impairment of joint function;
Grade III: the ligament is completely torn and loses its integrity, accompanied by significant swelling, bleeding and tenderness, accompanied by a marked loss of function and manifestations of joint instability.
IV. Clinical examination Front drawer test
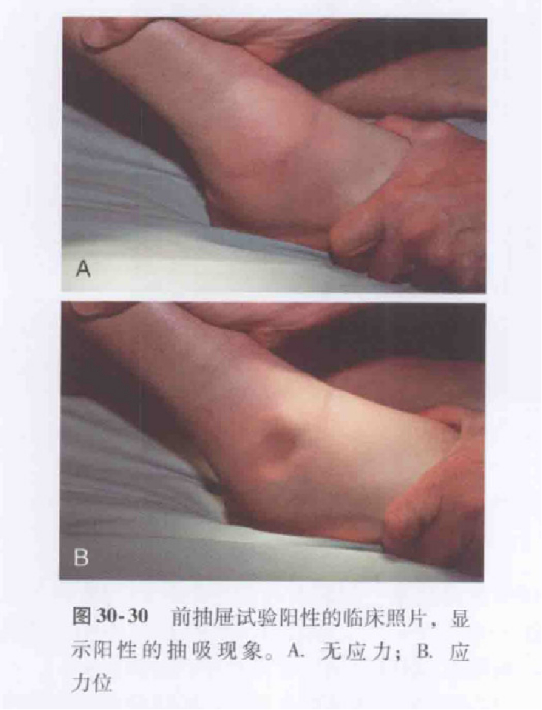
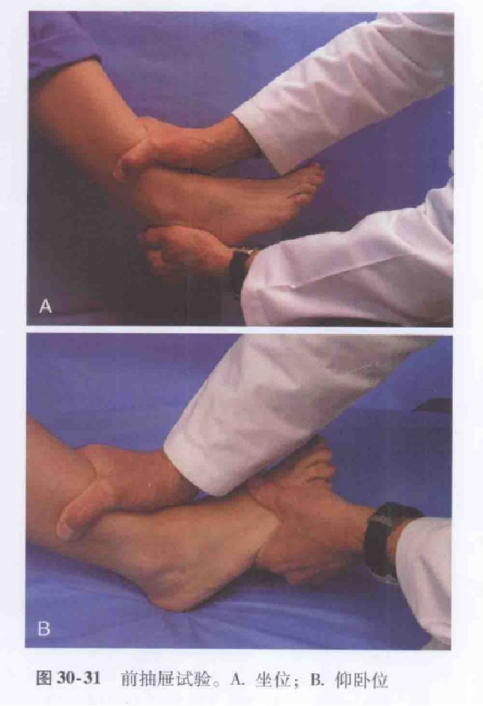
The patient is seated with the knee flexed and the end of the calf dangling, and the examiner holds the tibia in place with one hand and pushes the foot forward behind the heel with the other.
Alternatively, the patient is supine or seated with the knee bent at 60 to 90 degrees, the heel fixed to the ground, and the examiner applying posterior pressure to the distal tibia.
A positive predicts rupture of the anterior talofibular ligament.
Inversion stress test

The proximal ankle was immobilized, and varus stress was applied to the distal ankle to assess the talus tilt angle.
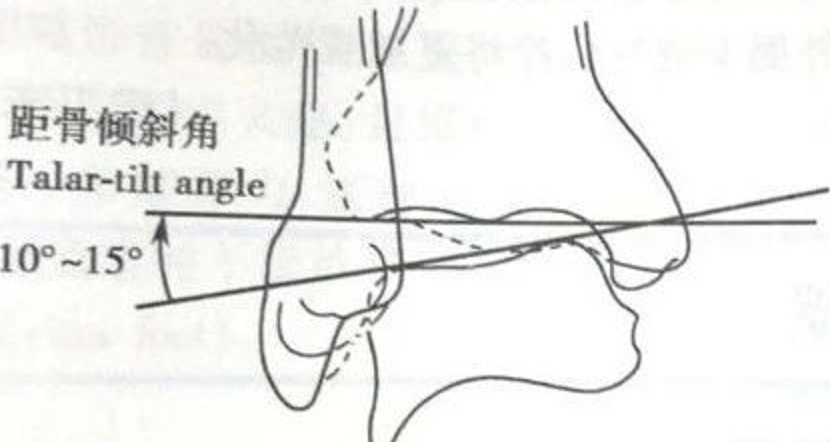
Compared with the contralateral side, >5° is suspiciously positive, and >10° is positive; or unilateral >15° is positive.
A positive predictor of calcaneofibular ligament rupture.
Imaging tests

X-rays of common ankle sports injuries
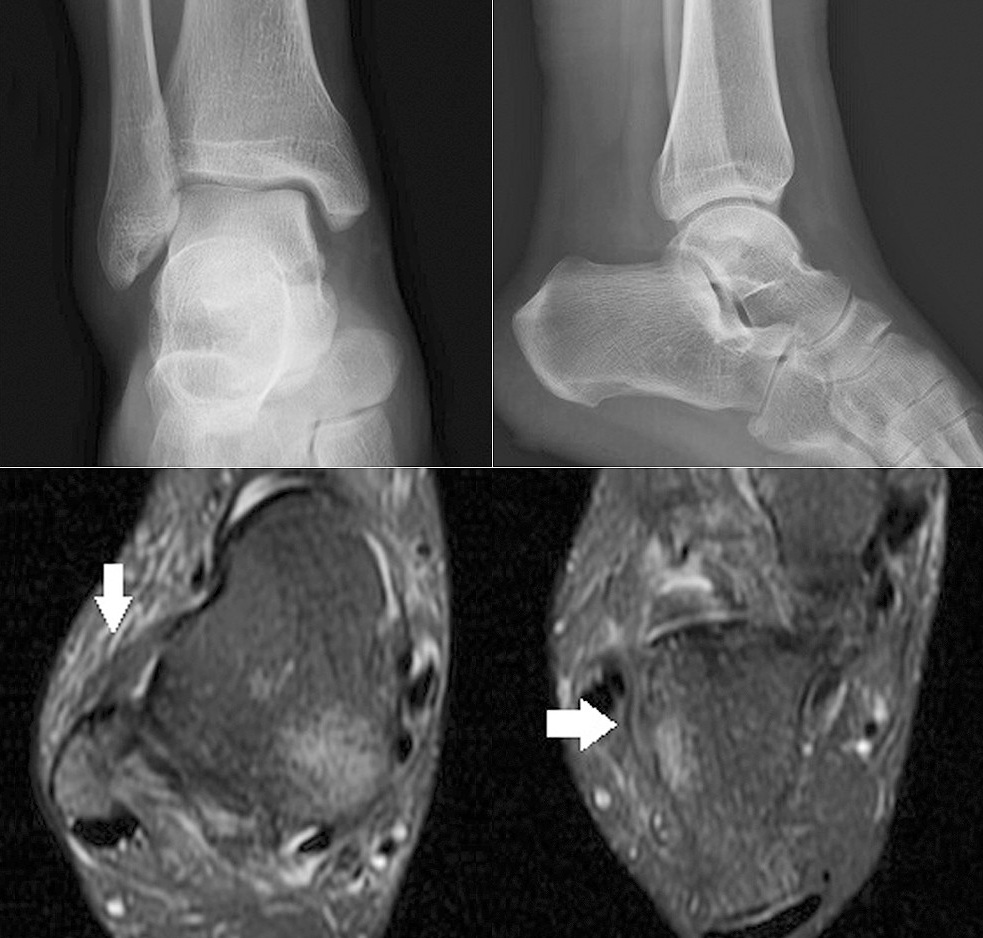
X-rays are negative, but MRI shows tears of the anterior talofibular and calcaneofibular ligaments
Advantages: X-ray is the first choice for examination, which is economical and simple; The extent of the injury is judged by judging the degree of talus inclination. Disadvantages: Poor display of soft tissues, especially the ligamentous structures that are important for maintaining joint stability.
MRI
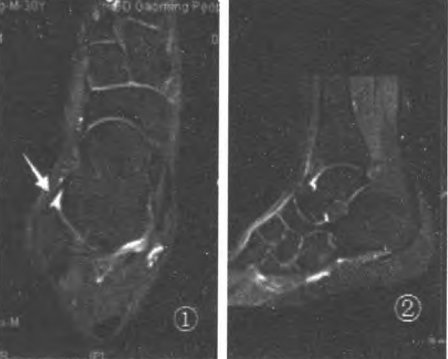
Fig.1 The 20° oblique position showed the best anterior talofibular ligament (ATFL); Fig.2 Azimuth line of ATFL scan
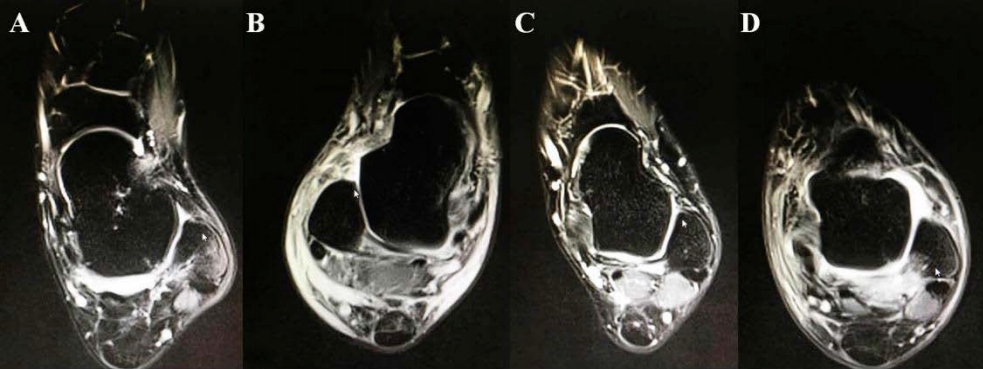
MRI images of different anterior talofibular ligament injuries showed that: (A) anterior talofibular ligament thickening and edema; (B) anterior talofibular ligament tear; (C) rupture of the anterior talofibular ligament; (D) Anterior talofibular ligament injury with avulsion fracture.
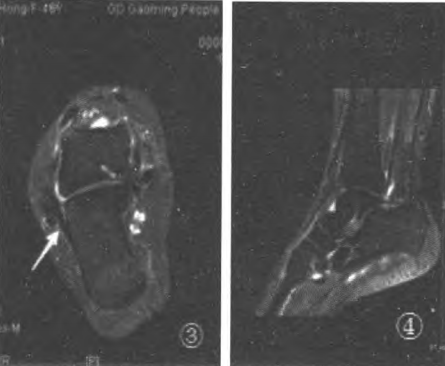
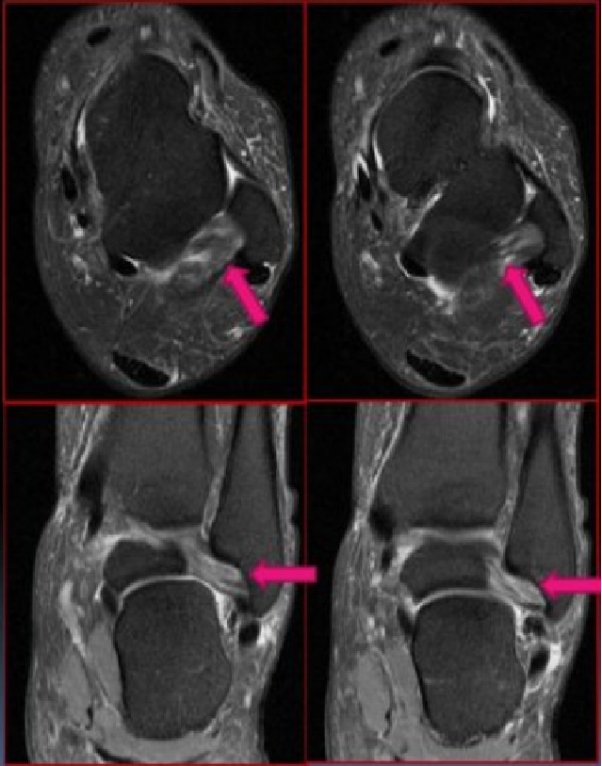
Fig.3 The -15° oblique position showed the best calcaneofibular ligament (CFI);
Fig.4. CFL scanning azimuth
Acute, complete tear of the calcaneofibular ligament
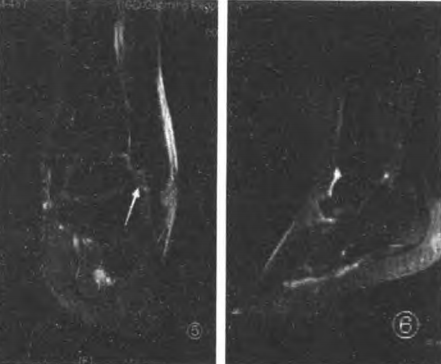
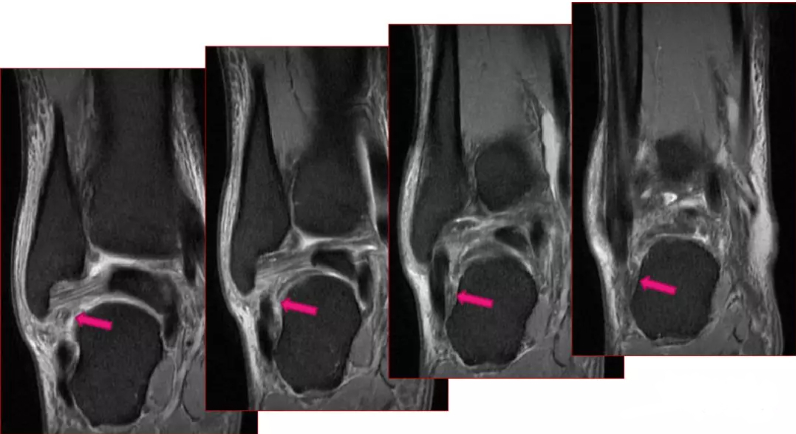
Figure 5: Coronal view shows the best posterior talofibular ligament (PTFL);
Fig.6 PTFL scan azimuth
Partial tear of the posterior talofibular ligament
Grading of diagnosis:
Class I: No damage;
Grade II: ligament contusion, good texture continuity, thickening of ligaments, hypoechogenicity, edema of surrounding tissues;
Grade III: incomplete ligament morphology, thinning or partial disruption of texture continuity, thickening of ligaments, and increased signal;
Grade IV: complete disruption of ligament continuity, which may be accompanied by avulsion fractures, thickening of ligaments, and increased local or diffuse signal.
Advantages: High resolution for soft tissues, clear observation of ligament injury types; It can show cartilage damage, bone contusion, and the overall condition of compound injury.
Disadvantages: It is not possible to accurately determine whether fractures and articular cartilage damage are interrupted; Due to the complexity of ankle ligament, the examination efficiency is not high; Expensive and time-consuming.
High-frequency ultrasound
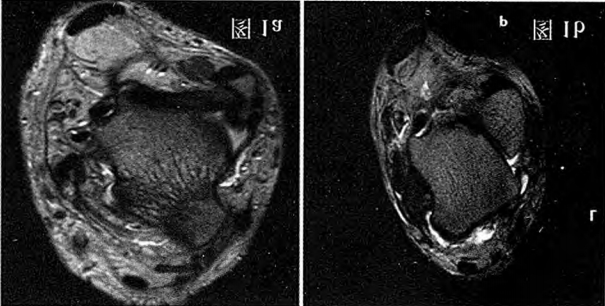
Figure 1a: Anterior talofibular ligament injury, partial tear; Figure 1b: The anterior talofibular ligament is completely torn, the stump is thickened, and a large effusion is seen in the anterior lateral space.
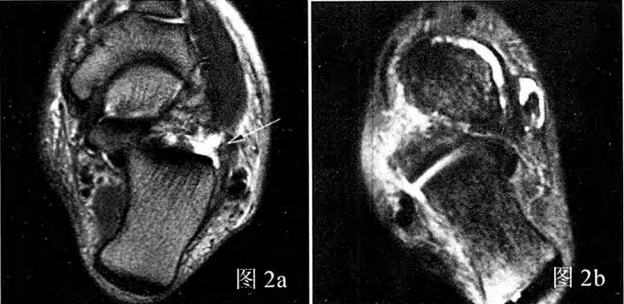
Figure 2a: Calcaneofibular ligament injury, partial tear; Figure 2b: Calcaneofibular ligament injury, complete rupture
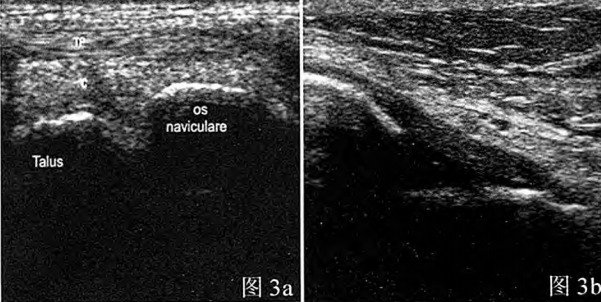
Figure 3a: Normal anterior talofibular ligament: ultrasound image showing an inverted triangle uniform hypoechoic structure; Figure 3b: Normal calcaneofibular ligament: Moderately echogenic and dense filamentous structure on ultrasound image
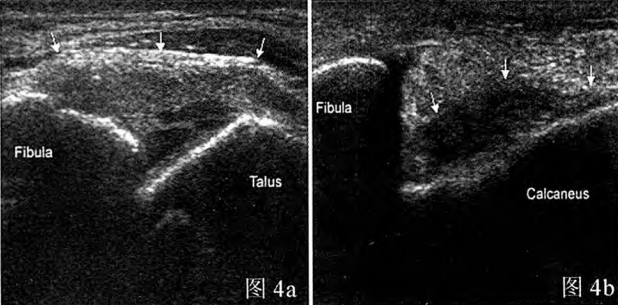
Figure 4a: Partial tear of the anterior talofibular ligament on ultrasound image; Figure 4b: Complete tear of the calcaneofibular ligament on ultrasound image
Grading of diagnosis:
contusion: acoustic images show intact structure, thickened and swollen ligaments; Partial tear: There is swelling in the ligament, there is persistent disruption of some fibers, or the fibers are locally thinned. Dynamic scans showed that the ligament tension was significantly weakened, and the ligament thinned and increased and the elasticity weakened in the case of valgus or varus.
Complete tear: a completely and persistently interrupted ligament with distal separation, dynamic scan suggests no ligament tension or increased tear, and in valgus or varus, the ligament moves to the other end, without any elasticity and with a loose joint.
Advantages: low cost, easy to operate, non-invasive; The subtle structure of each layer of subcutaneous tissue is clearly displayed, which is conducive to the observation of musculoskeletal tissue lesions. Arbitrary section examination, according to the ligament belt to trace the whole process of ligament, the location of ligament injury is clarified, and the ligament tension and morphological changes are dynamically observed.
Disadvantages: lower soft-tissue resolution compared to MRI; Rely on professional technical operation.
Arthroscopy check

Advantages: Directly observe the structures of the lateral malleolus and hindfoot (such as the inferior talar joint, anterior talofibular ligament, calcaneofibular ligament, etc.) to evaluate the integrity of the ligaments and help the surgeon determine the surgical plan.
Disadvantages: Invasive, may cause some complications, such as nerve damage, infection, etc. It is generally considered to be the gold standard for diagnosing ligament injuries and is currently mostly used in the treatment of ligament injuries.
Post time: Sep-29-2024





