




"10% of ankle fractures are accompanied by distal tibiofibular syndesmosis injury. Studies have shown that 52% of distal tibiofibular screws result in poor reduction of the syndesmosis. Inserting the distal tibiofibular screw perpendicular to the syndesmosis joint surface is essential to avoid iatrogenic malreduction. According to the AO manual, it is recommended to insert the distal tibiofibular screw 2 cm or 3.5 cm above the distal tibial articular surface, at an angle of 20-30° to the horizontal plane, from the fibula to the tibia, with the ankle in a neutral position."
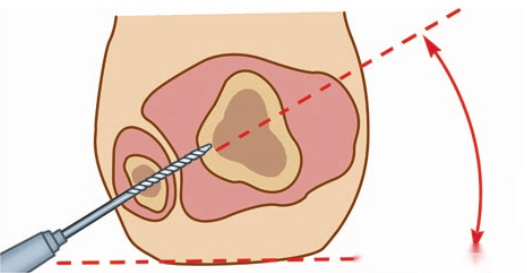
Manual insertion of distal tibiofibular screws often results in deviations in the entry point and direction, and currently, there is no precise method for determining the insertion direction of these screws. To address this issue, foreign researchers have adopted a new method—the 'angle bisector method.
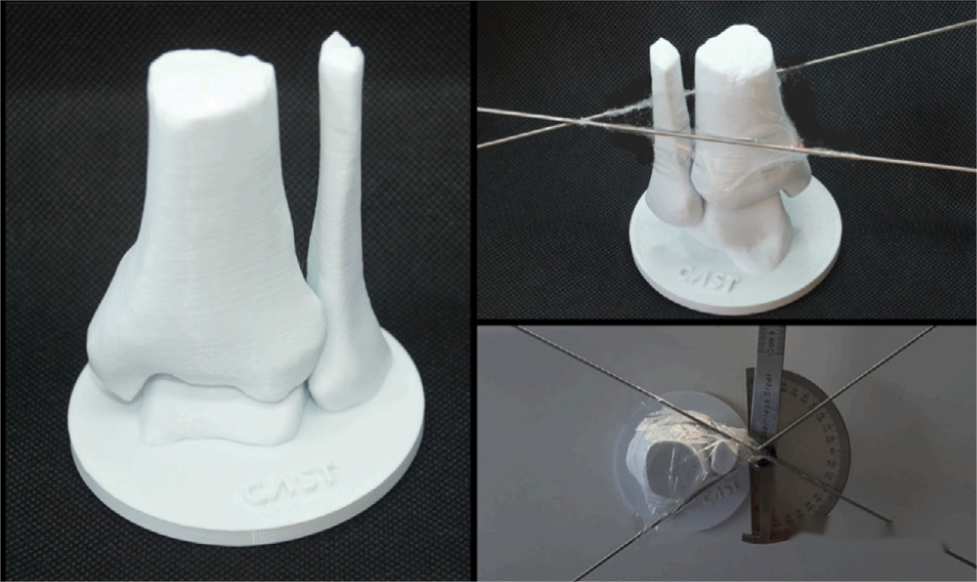
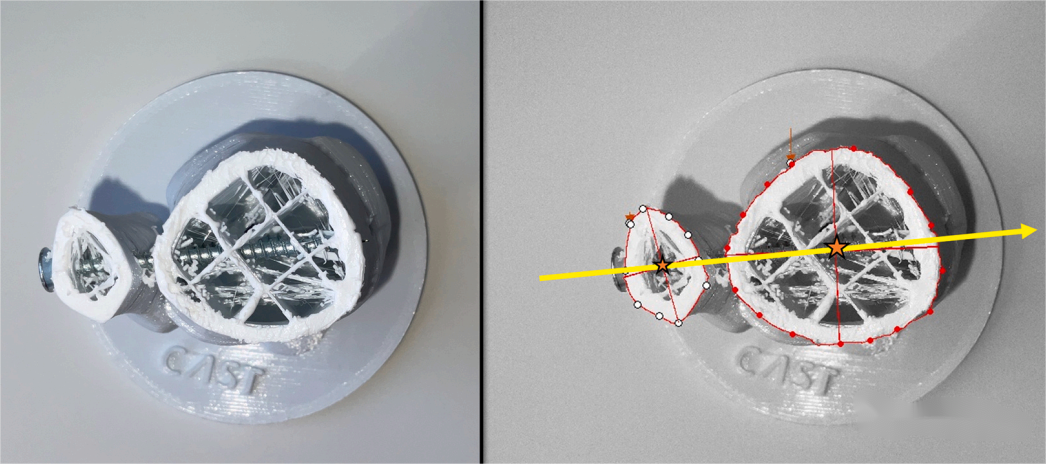
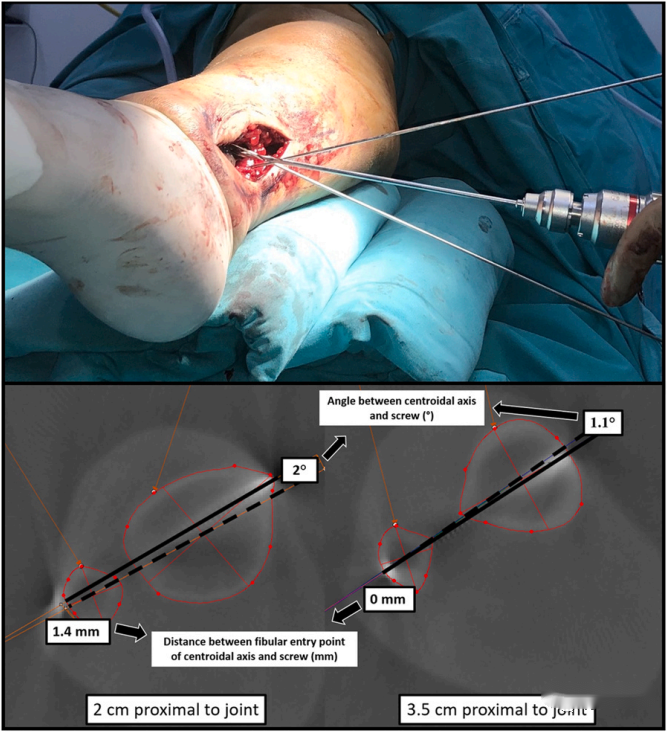
Using imaging data from 16 normal ankle joints, 16 3D-printed models were created. At distances of 2 cm and 3.5 cm above the tibial articular surface, two 1.6 mm Kirschner wires parallel to the joint surface were placed close to the anterior and posterior edges of the tibia and fibula, respectively. The angle between the two Kirschner wires was measured using a protractor, and a 2.7 mm drill bit was used to drill a hole along the angle bisector line, followed by the insertion of a 3.5 mm screw. After screw insertion, the screw was cut along its length using a saw to evaluate the relationship between the screw direction and the central axis of the tibia and fibula.

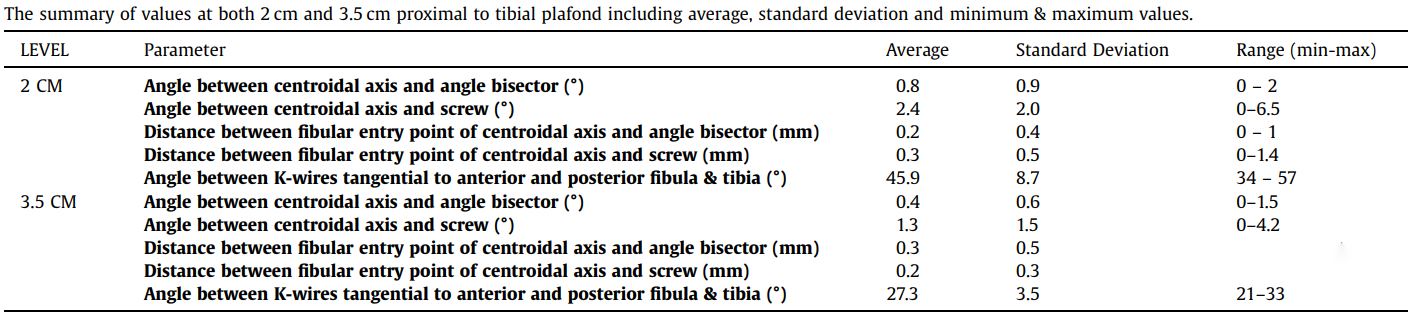
Specimen experiments indicate that there is a good consistency between the central axis of the tibia and fibula and the angle bisector line, as well as between the central axis and the screw direction.
heoretically, this method can effectively place the screw along the central axis of the tibia and fibula. However, during surgery, placing the Kirschner wires close to the anterior and posterior edges of the tibia and fibula poses a risk of damaging blood vessels and nerves. Additionally, this method does not resolve the issue of iatrogenic malreduction, as the distal tibiofibular alignment cannot be adequately assessed intraoperatively before screw placement.
Post time: Jul-30-2024





