




Currently, the most commonly used surgical approach for calcaneal fractures involves internal fixation with plate and screw through the sinus tarsi entry route. The lateral “L” shaped expanded approach is no longer preferred in clinical practice due to higher wound-related complications. The plate and screw system fixation, due to its biomechanical characteristics of eccentric fixation, carries a higher risk of varus malalignment, with some studies indicating a postoperative probability of secondary varus of about 34%.
As a result, researchers have begun studying intramedullary fixation methods for calcaneal fractures to address both wound-related complications and the issue of secondary varus malalignment.
01 Nail central nailing technique
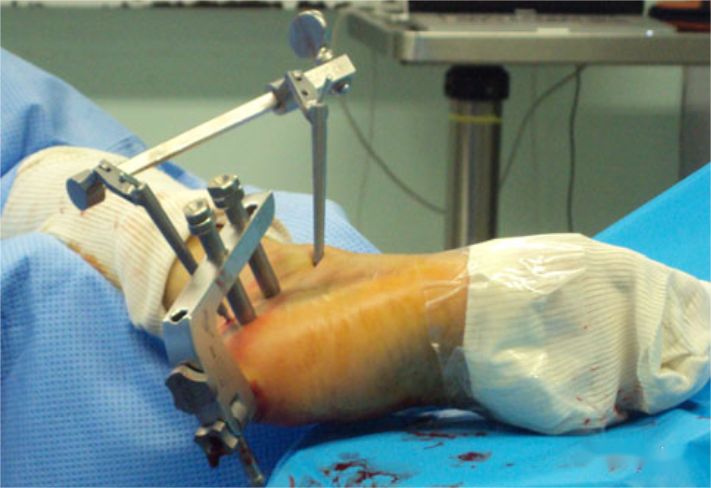
This technique can assist in reduction through the sinus tarsi entry route or under arthroscopic guidance, requiring lower soft tissue demands and potentially reducing hospitalization time. This approach is selectively applicable to type II-III fractures, and for complex comminuted calcaneal fractures, it might not provide strong maintenance of reduction and may require additional screw fixation.


02 Single-plane intramedullary nail
The single-plane intramedullary nail features two screws at the proximal and distal ends, with a hollow main nail that allows for bone grafting through the main nail.
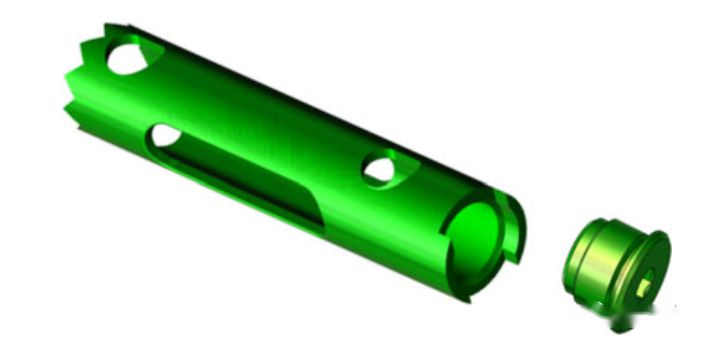

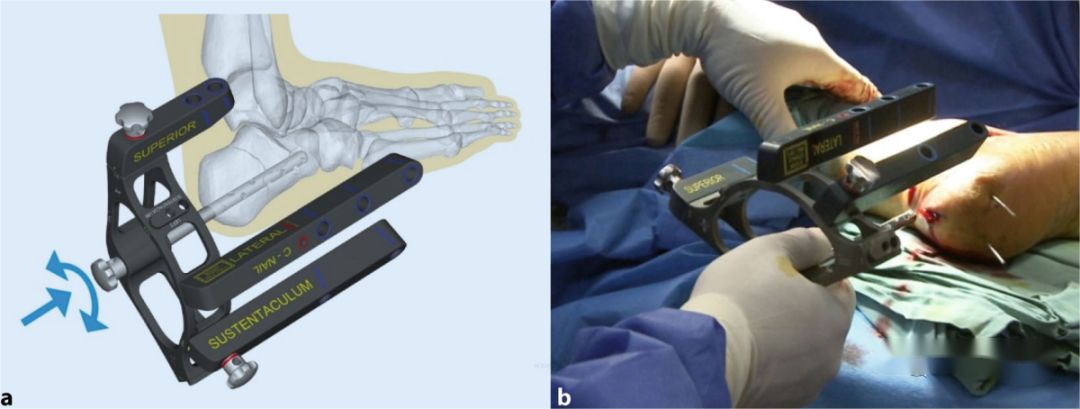
03 Multi-plane intramedullary nail
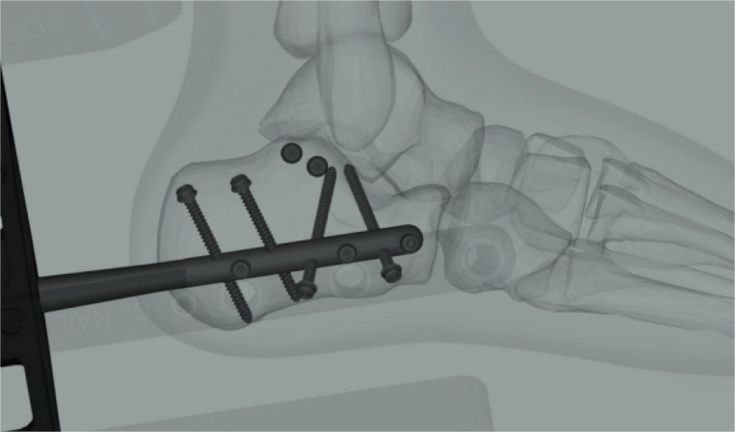
Designed based on the three-dimensional structural morphology of the calcaneus, this internal fixation system includes key screws such as load-bearing protrusion screws and posterior process screws. After reduction through the sinus tarsi entry route, these screws can be placed under the cartilage for support.

There are several controversies regarding the use of intramedullary nails for calcaneal fractures:
1. Suitability based on fracture complexity: It is debated whether simple fractures do not require intramedullary nails and complex fractures are not suitable for them. For Sanders type II/III fractures, the technique of reduction and screw fixation through the sinus tarsi entry route is relatively mature, and the significance of the main intramedullary nail may be questioned. For complex fractures, the advantages of the “L” shaped expanded approach remain irreplaceable, as it provides sufficient exposure.
2. Necessity of an artificial medullary canal: The calcaneus naturally lacks a medullary canal. Using a large intramedullary nail might result in excessive trauma or loss of bone mass.
3. Difficulty in removal: In many cases in China, patients still undergo hardware removal after fracture healing. The nail’s integration with bone growth and embedding of lateral screws under the cortical bone can lead to difficulty in removal, which is a practical consideration in clinical applications.
Post time: Aug-23-2023





