




Currently, distal radius fractures are treated in various ways, such as plaster fixation, incision and reduction internal fixation, external fixation bracket, etc. Among them, palmar plate fixation can achieve more satisfactory results, but some literature reports that its complication rate is as high as 16%. However, if the plate is properly selected, the complication rate can be effectively reduced. A brief overview of the types, indications and surgical techniques of palmar plating for distal radius fractures is presented.
I.Types of distal radius fractures
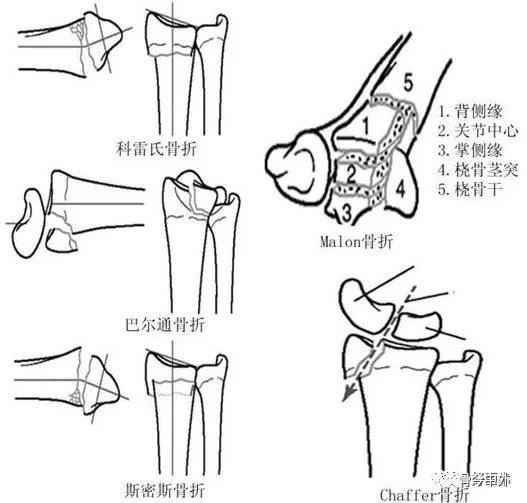
There are several classification systems for fractures, including the Müller AO classification based on anatomy and the Femandez classification based on mechanism of injury. Among them, the Eponymic classification combines the advantages of previous classifications, covers the four basic types of fractures, and includes Maleon 4-part fractures and Chaffer's fractures, which can be a good guide for clinical work.
1. Müller AO classification - partial intra-articular fractures
The AO classification is well suited to distal radius fractures and divides them into three main types: type A extra-articular, type B partial intra-articular, and type C total joint fractures. Each type is further divided into different combinations of subgroups based on the severity and complexity of the fracture.
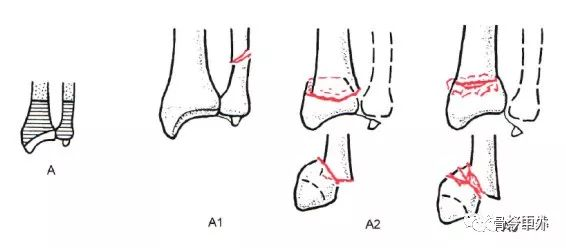
Type A:Extra-articular fracture
A1, ulnar femoral fracture, radius as injury (A1.1, ulnar stem fracture; A1.2 simple fracture of the ulnar diaphysis; A1.3, comminuted fracture of the ulnar diaphysis).
A2, Fracture of radius, simple, with inset (A2.1, radius without tilt; A2.2, dorsal tilt of radius, i.e., Pouteau-Colles fracture; A2.3, palmar tilt of radius, i.e., Goyrand-Smith fracture).
A3, Fracture of the radius, comminuted (A3.1, axial shortening of the radius; A3.2 wedge-shaped fragment of the radius; A3.3, comminuted fracture of the radius).
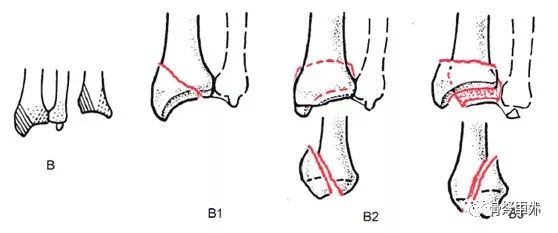
Type B: partial articular fracture
B1, fracture of the radius, sagittal plane (B1.1, lateral simple type; B1.2, lateral comminuted type; B1.3, medial type).
B2, Fracture of the dorsal rim of the radius, i.e., Barton fracture (B2.1, simple type; B2.2, combined lateral sagittal fracture; B2.3, combined dorsal dislocation of the wrist).
B3, Fracture of the metacarpal rim of the radius, i.e., an anti-Barton fracture, or a Goyrand-smith type II fracture (B3.1, simple femoral rule, small fragment; B3.2, simple fracture, large fragment; B3.3, comminuted fracture).
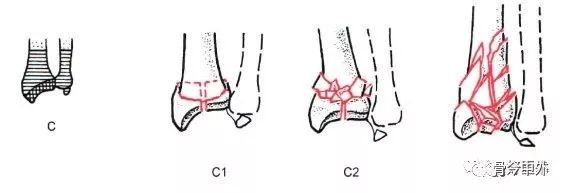
Type C: total articular fracture
C1, radial fracture with simple type of both articular and metaphyseal surfaces (C1.1, posterior medial articular fracture; C1.2, sagittal fracture of articular surface; C1.3, fracture of coronal surface of articular surface).
C2, Radius fracture, simple articular facet, comminuted metaphysis (C2.1, sagittal fracture of articular facet; C2.2, coronal facet fracture of articular facet; C2.3, articular fracture extending into radial stem).
C3, radial fracture, comminuted (C3.1, simple fracture of metaphysis; C3.2, comminuted fracture of metaphysis; C3.3, articular fracture extending to radial stem).
2.Classification of distal radius fractures.
According to the mechanism of injury Femandez classification can be divided into 5 types:.
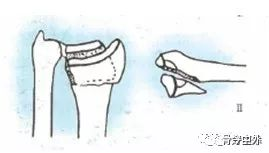
Type I fractures are extra-articular metaphyseal comminuted fractures such as Colles fractures (dorsal angulation) or Smith fractures (metacarpal angulation). The cortex of one bone breaks under tension and the contralateral cortex is comminuted and embedded.
Fracture
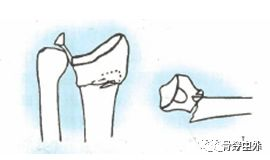
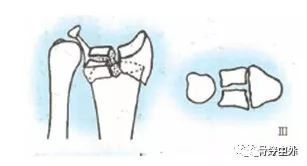
Type III fractures are intra-articular fractures, caused by shear stress. These fractures include palmar Barton fractures, dorsal Barton fractures, and radial stem fractures.
Shear stress
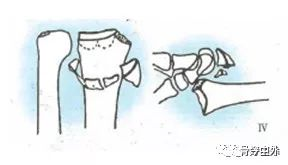
Type III fractures are intra-articular fractures and metaphyseal insertions caused by compression injuries, including complex articular fractures and radial pilon fractures.
Insertion
Type IV fracture is an avulsion fracture of the ligamentous attachment that occurs during fracture-dislocation of the radial carpal joint.
Avulsion fracture I dislocation
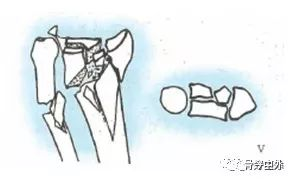
Type V fracture arises from a high velocity injury involving multiple external forces and extensive injuries. (Mixed I, II, IIII, IV)
3.Eponymic typing
II.Treatment of distal radius fractures with palmar plating
Indications.
For extra-articular fractures following failure of closed reduction in the following conditions.
Dorsal angulation greater than 20°
Dorsal compression greater than 5 mm
Distal radius shortening greater than 3 mm
Distal fracture block displacement greater than 2 mm
For intra-articular fractures greater than 2mm displacement
Most scholars do not recommend the use of metacarpal plates for high-energy injuries, such as severe intra-articular comminuted fractures or severe bone loss, because these distal fracture fragments are prone to avascular necrosis and are difficult to anatomically reposition.
In patients with multiple fracture fragments and significant displacement with severe osteoporosis, metacarpal plating is not effective. The subchondral support of distal fractures may be problematic, such as screw penetration into the joint cavity.
Surgical technique
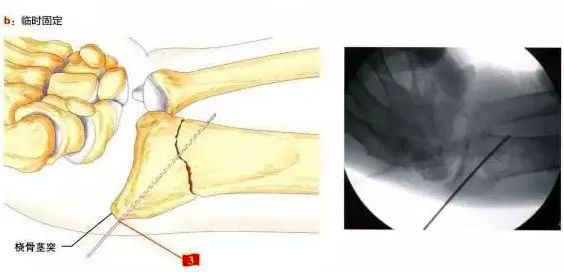
Most surgeons use a similar approach and technique for fixing distal radius fractures with a palmar plate. However, a good surgical technique is required to effectively avoid postoperative complications, e.g., reduction can be achieved by releasing the fracture block from embedded compression and restoring continuity of the cortical bone. Temporary fixation with 2-3 Kirschner pins may be used, etc.
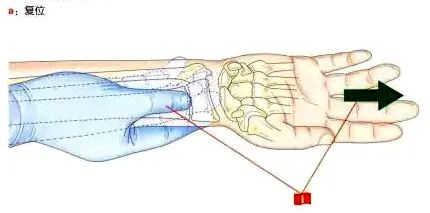
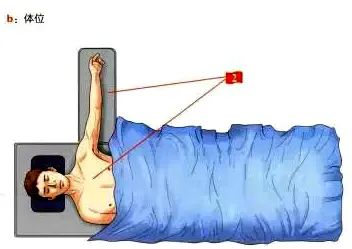
(I) Preoperative repositioning and posture
1. Traction is performed in the direction of the radial shaft under fluoroscopy, with the thumb pressing the proximal fracture block down from the palmar side and the other fingers lifting the distal block up at an angle from the dorsal side.
2. Supine position, with the affected limb on a hand table under fluoroscopy.
(II) Access points.
For the type of approach to be used, the PCR (radial carpal flexor) extended palmar approach is recommended.
The distal end of the skin incision begins in the skin crease of the wrist and its length can be determined according to the type of fracture.
The radial flexor carpi radialis tendon and its tendon sheath are incised, distal to the carpal bones and proximal as close to the proximal side as possible.
Pulling the radial carpal flexor tendon to the ulnar side protects the median nerve and flexor tendon complex.
The Parona space is exposed and the anterior rotator ani muscle is located between the flexor digitorum longus (ulnar side) and the radial artery (radial side).
Incise the radial side of the anterior rotator ani muscle, noting that a portion should be left attached to the radius for later reconstruction.
Pulling the anterior rotator ani muscle to the ulnar side allows for more adequate exposure of the ulnar horn on the palmar side of the radius.

The palmar approach exposes the distal radius and effectively exposes the ulnar angle.
For complex fracture types, it is recommended that the distal brachioradialis stop can be released, which can neutralise its pull on the radial tuberosity, at which point the palmar sheath of the first dorsal compartment can be incised, which can expose the distal fracture block radial and radial tuberosity, internally rotate the radius Yu to disengage it from the fracture site, and then reset the intra-articular fracture block using a Kirschner pin. For complex intra-articular fractures, arthroscopy can be used to assist in the reduction, evaluation and fine-tuning of the fracture block.
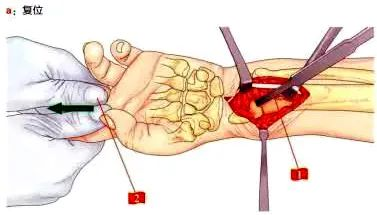
(III) Methods of reduction.
1. Use the bone pry as a lever for resetting
2. The assistant pulls the patient's index and middle fingers, which will be relatively easy to reset.
3. Screw the Kirschner pin from the radial tuberosity for temporary fixation.
After repositioning is complete, a palmar plate is routinely placed, which must be just close to the watershed, must cover the ulnar eminence, and should be proximal to the midpoint of the radial stem. If these conditions are not met, if the plate is not the right size, or if the repositioning is unsatisfactory, the procedure is still not perfect.
Many complications are strongly related to the position of the plate. If the plate is placed too far to the radial side, complications related to the bunion flexor are likely to occur; if the plate is placed too close to the watershed line, the deep flexor of the finger may be at risk. Displaced deformity of the fracture repositioning to the palmar side can easily cause the plate to protrude to the palmar side and come into direct contact with the flexor tendon, eventually leading to tendonitis or even rupture.
In osteoporotic patients, it is recommended that the plate be placed as close to the watershed line as possible, but not across it. Subchondral fixation can be achieved using Kirschner pins closest to the ulna, and side-by-side Kirschner pins and locking screws are effective in avoiding fracture redisplacement.
Once the plate is correctly placed, the proximal end is fixed with one screw and the distal end of the plate is temporarily fixed with Kirschner pins in the most ulnar hole. Intraoperative fluoroscopic orthopantomograms, lateral views, and lateral films with 30° wrist elevation were taken to determine the fracture reduction and the position of the internal fixation.
If the plate is satisfactorily positioned, but the Kirschner pin is intra-articular, this will result in inadequate recovery of the palmar inclination, which can be resolved by resetting the plate using the "distal fracture fixation technique" (Fig. 2, b).
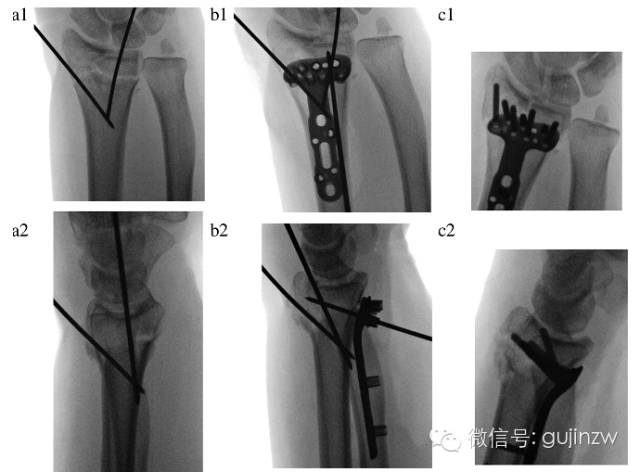
Figure 2.
a, two Kirschner pins for temporary fixation, note that the metacarpal inclination and articular surfaces are not sufficiently restored at this point;
b, One Kirschner pin for temporary plate fixation, note that the distal radius is fixed at this point (distal fracture block fixation technique), and the proximal portion of the plate is pulled toward the radial stem to restore the palmar tilt angle.
C, Arthroscopic fine-tuning of the articular surfaces, placement of distal locking screws/pins, and final resetting and fixation of the proximal radius.
In the case of concomitant dorsal and ulnar fractures (ulnar/dorsal Die Punch), which cannot be adequately reset under closure, the following three techniques may be used.
The proximal radius is rotated anteriorly away from the fracture site, and the fracture block of the lunate fossa is pushed towards the carpal bone through a PCR lengthening approach; a small incision is made dorsal to the 4th and 5th compartments to expose the fracture block, and it is screw-fixed in the plate's most ulnar foramen. Closed percutaneous or minimally invasive fixation was performed with arthroscopic assistance.
After satisfactory repositioning and correct placement of the plate, final fixation is simpler and anatomical repositioning can be achieved if the proximal ulnar kernel pin is correctly positioned and no screws are in the joint cavity (Figure 2).
(iv) Screw selection experience.
The length of the screws may be difficult to measure accurately due to the severe dorsal cortical bone crush. Screws that are too long may lead to tendon agitation and too short to support fixation of the dorsal fracture block. For this reason the authors recommend the use of threaded locking nails and multiaxial locking nails in the radial tuberosity and most ulnar foramen, and the use of light-stem locking screws in the remaining positions. The use of a blunt head avoids agitation of the tendon even if it is threaded dorsally. For proximal interlocking plate fixation, two interlocking screws + one common screw (placed through an ellipse) can be used for fixation.
Dr Kiyohito from France presented their experience of using minimally invasive palmar locking plates for distal radius fractures, where their surgical incision was reduced to an extreme 1cm, which is counterintuitive. This method is primarily indicated for relatively stable distal radius fractures, and its surgical indications are for extra-articular fractures of AO fractions of types A2 and A3 and intra-articular fractures of types C1 and C2, but it is not suitable for C1 and C2 fractures combined with intra-articular bone mass collapse. The method is also not suitable for type B fractures. The authors also point out that if good reduction and fixation cannot be achieved with this method, it is necessary to switch to the traditional incision method and not to stick to the minimally invasive small incision.
Post time: Jun-26-2024





