




Operating Method
(I) Anaesthesia
Brachial plexus block is used for the upper limbs, epidural block or subarachnoid block is used for the lower limbs, and general anaesthesia or local anaesthesia can also be used as appropriate.
(II) Position
Upper limbs: supine, elbow flexion, forearm in front of chest.
Lower limbs: supine, hip flexion, abduction, knee flexion and ankle joint in 90 degree dorsal extension position.
(III)Operation sequence
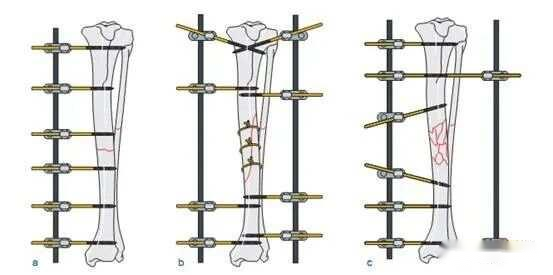
The specific sequence of operation of the external fixator is an alternation of resetting, threading and fixation.
[Procedure]
That is, the fracture is first initially repositioned (correcting rotational and overlapping deformities), then pierced with pins distal to the fracture line and initially fixed, then further repositioned and pierced with pins proximal to the fracture line, and finally repositioned to the satisfaction of the fracture and then fixed in its entirety. In some special cases, the fracture can also be fixed by direct pinning, and when the situation permits, the fracture can be repositioned, adjusted and re-fixed.
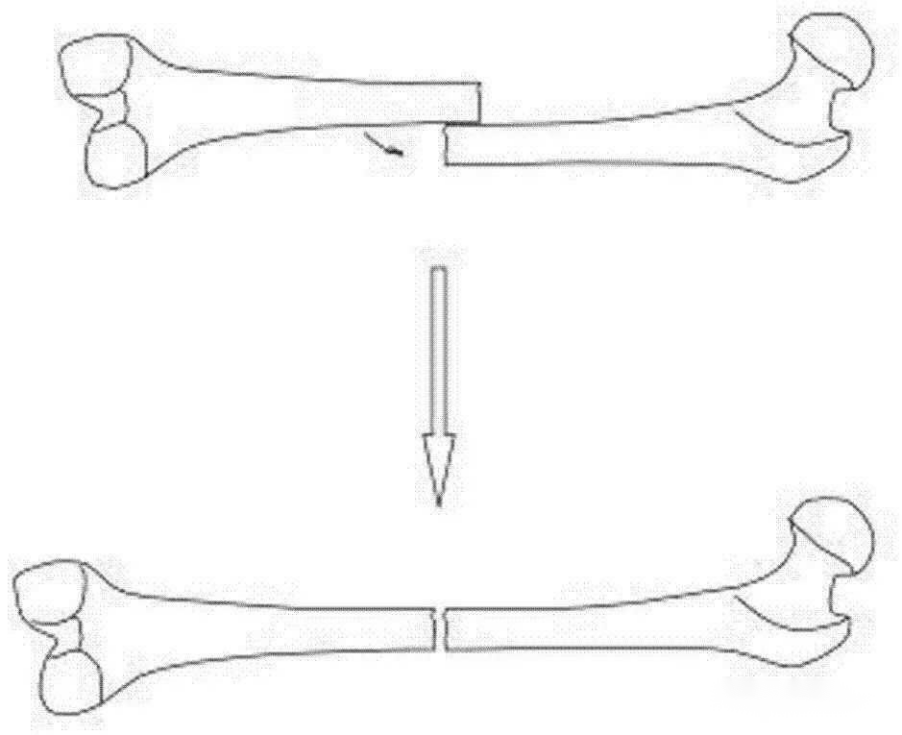
[Fracture Reduction]
Fracture reduction is a key part of fracture treatment. Whether the fracture is satisfactorily reduced has a direct impact on the quality of fracture healing. The fracture can be closed or under direct vision according to the specific situation. It can also be adjusted according to the X-ray film after the body surface marking. The specific methods are as follows.
1. Under direct vision: For open fractures with exposed fracture ends, the fracture can be reset under direct vision after thorough debridement. If the closed fracture fails manipulation, the fracture can also be reduced, pierced and fixed under direct vision after a small incision of 3~5cm.
2. Closed reduction method: first make the fracture roughly reset and then operate according to the sequence, can use the steel pin near the fracture line, and apply the method of lifting and wrenching to assist the fracture to be further reset until it is satisfied and then fixed. It is also possible to make appropriate adjustments for small displacement or angulation according to X-ray after approximate reduction and fixation based on the body surface or bony markings. Requirements for fracture reduction, in principle, is anatomical reduction, but serious comminuted fracture, often not easy to restore the original anatomical form, at this time the fracture should be better contact between the fracture block, and to maintain a good force line requirements.
[Pinning]
Pinning is the main operation technique of external bone fixation, and the good or bad technique of pinning not only affects the stability of fracture fixation, but also relates to the high or low incidence of comorbidity. Therefore, the following operation techniques should be strictly followed when threading the needle.
1. Avoid collateral damage: Fully understand the anatomy of the piercing site and avoid injuring the main blood vessels and nerves.
2. Strictly aseptic operation technique, the needle should be 2~3cm outside the infected lesion area.
3. Strictly non-invasive techniques: when wearing half-needle and thick diameter full needle, the inlet and outlet of the steel needle with a sharp knife to make a 0.5~1cm skin incision; when wearing half-needle, use haemostatic forceps to separate the muscle and then place the cannula and then drill holes. Do not use high-speed power drilling when drilling or directly threading the needle. After threading the needle, the joints should be moved to check whether there is any tension in the skin at the needle, and if there is tension, the skin should be cut and sutured.
4. Correctly select the location and angle of the needle: the needle should not pass through the muscle as little as possible, or the needle should be inserted in the muscle gap: when the needle is inserted in a single plane, the distance between the needles in a fracture segment should not be less than 6 cm; when the needle is inserted in multiple planes, the distance between the needles in a fracture segment should be as large as possible. The distance between the pins and the fracture line or articular surface should not be less than 2cm.The crossing angle of the pins in multiplanar needling should be 25°~80° for full pins and 60°~80° for half pins and full pins.
5. Correctly select the type and diameter of the steel needle.
6. Wrap the needle hole flatly with alcohol gauze and sterile gauze.
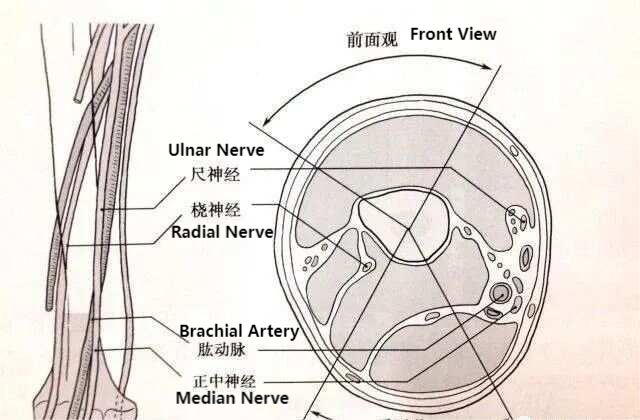
Position of the distal humeral penetrating needle in relation to the vascular nerve bundle of the upper arm (The sector shown in the illustration is the safety zone for threading the needle.)
[Mounting and fixation]
In most cases fracture reduction, pinning and fixation are carried out alternately, and fixation is completed as required when the predetermined steel pins have been pierced. Stable fractures are fixed with compression (but the force of compression should not be too great, otherwise angular deformity will occur), comminuted fractures are fixed in the neutral position, and bone defects are fixed in the distraction position.
The fashion of overall fixation should pay attention to the following issues: 1.
1. Test the stability of fixation: the method is to manoeuvre the joint, longitudinal drawing or lateral pushing the fracture end; the stable fixed fracture end should have no activity or only a small amount of elastic activity. If the stability is insufficient, appropriate measures can be taken to increase the overall stiffness.
2. The distance from the bone external fixator to the skin: 2~3cm for the upper limb, 3~5cm for the lower limb, in order to prevent skin compression and facilitate trauma treatment, when the swelling is serious or the trauma is large, the distance can be left larger in the early stage, and the distance can be reduced after the swelling subsides and the trauma is repaired.
3. When accompanied by serious soft tissue injury, some parts can be added to make the injured limb suspended or overhead, in order to facilitate the swelling of the limb and prevent pressure injury.
4. The bone external fixator of the bone cadre should not affect the functional exercise of the joints, the lower limb should be easy to walk under load, and the upper limb should be easy for daily activities and self-care.
5. The end of the steel needle can be exposed to the steel needle fixation clip for about 1cm, and the excessively long tail of the needle should be cut off. The end of the needle with a plastic cap seal or tape wrapped, so as not to puncture the skin or cut the skin.
[Steps to be taken in special cases]
For patients with multiple injuries, due to serious injuries or life-threatening injuries during resuscitation, as well as in emergency situations such as first aid in the field or batch injuries, the needle can be threaded and secured first, and then re-corrected, adjusted, and secured at the appropriate time.
[Common Complications]
1. Pinhole infection; and
2. Skin compression necrosis; and
3. Neurovascular injury
4. Delayed healing or non-healing of fracture.
5. Broken pins
6. Pin tract fracture
7. Joint dysfunction
(IV) Post-operative treatment
Proper postoperative treatment directly affects the efficacy of treatment, otherwise complications such as pinhole infection and non-union of fracture may occur. Therefore, adequate attention should be paid.
[General treatment]
After the operation, the injured limb should be elevated, and the blood circulation and swelling of the injured limb should be observed; when the skin is compressed by the components of the bone external fixator due to the position or swelling of the limb, it should be handled in time. Loose screws should be tightened in time.
[Preventing and treating infections]
For external bone fixation itself, antibiotics are not necessary to prevent pinhole infection. However, the fracture and the wound itself must still be treated with antibiotics as appropriate. For open fractures, even if the wound is thoroughly debrided, antibiotics should be applied for 3 to 7 days, and infected fractures should be given antibiotics for a longer period of time as appropriate.
[Pinhole care]
More work after external bone fixation is required to care for pinholes on a regular basis. Improper pinhole care will result in pinhole infection.
1. Generally the dressing is changed once on the 3rd day after surgery, and the dressing needs to be changed every day when there is oozing from the pinhole.
2. 10 days or so, the skin of the pinhole is fibrous wrapped, while keeping the skin clean and dry, every 1~2 days in the pinhole skin drops of 75% alcohol or iodine fluoride solution can be.
3. When there is tension in the skin at the pinhole, the tension side should be cut in time to reduce the tension.
4. Pay attention to the aseptic operation when adjusting the bone external fixator or changing the configuration, and disinfect the skin around the pinhole and the steel needle routinely.
5. Avoid cross-infection during pinhole care.
6. Once pinhole infection occurs, correct surgical treatment should be carried out in time, and the injured limb should be elevated for rest and appropriate antimicrobials should be applied.
[Functional exercise]
Timely and correct functional exercise is not only conducive to the recovery of joint function, but also to the reconstruction of haemodynamics and stress stimulation to promote the process of fracture healing. Generally speaking, muscle contraction and joint activities can be carried out in bed within 7 days after the operation. The upper limbs can carry out pinching and holding of the hands and autonomous movements of the wrist and elbow joints, and rotational exercises can be started 1 week later; the lower limbs can partially leave the bed with the help of crutches after 1 week or after the wound has healed, and then gradually start walking with full weight-bearing 3 weeks later. The timing and mode of functional exercise varies from person to person, mainly depending on the local and systemic conditions. In the process of exercise, if the pinhole appears red, swollen, painful and other inflammatory manifestations should stop the activity, elevate the affected limb to bed rest.
[Removal of external bone fixator]
The external fixation brace should be removed when the fracture has reached the clinical criteria for fracture healing. When removing the external bone fixation bracket, the healing strength of the fracture should be accurately determined, and the external bone fixation should not be removed prematurely without the certainty of determining the healing strength of the bone and obvious complications of the external bone fixation, especially when treating conditions such as old fracture, comminuted fracture, and bone nonunion.
Post time: Aug-29-2024





