




When choosing a treatment plan for distal tibial fractures, external fixation can be used as a temporary fixation for fractures with severe soft tissue injuries.
Indications:
“Damage control” temporary fixation of fractures with significant soft tissue injury, such as open fractures or closed fractures with significant soft tissue swelling.
Definitive treatment of contaminated, infected fractures, or fractures with severe soft tissue injury.
Examine:
Soft tissue condition: ①Open wound; ②Severe soft tissue contusion, soft tissue swelling. Check for neurovascular status and carefully record.
Imaging: Anteroposterior and lateral X-rays of the tibia, and anteroposterior, lateral and ankle acupoints of the ankle joint. If an intra-articular fracture is suspected, a CT scan of the tibial vault should be performed.

Anatomy:·
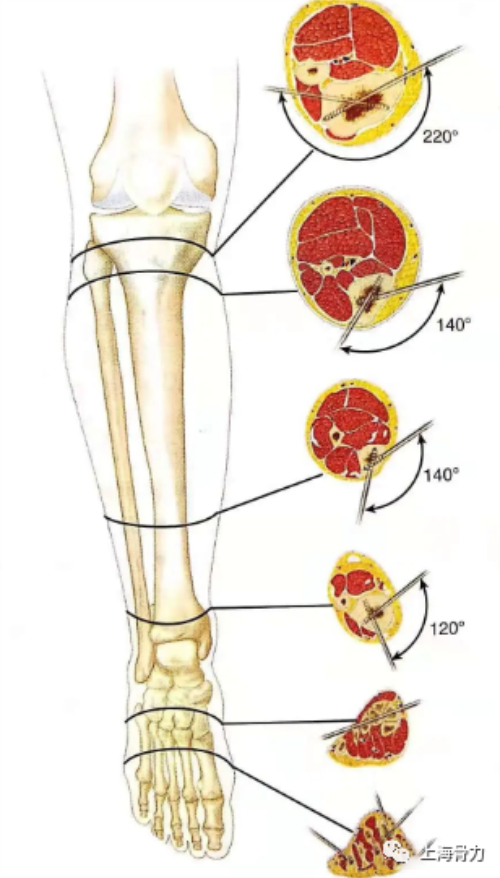
The anatomical “safe zone” for external fixation pin placement was defined according to different levels of cross-section.
The proximal metaphysis of the tibia provides a 220° anterior arc-shaped safety zone where external fixation pins can be placed.
Other parts of the tibia provide an anteromedial safe needle insertion area in the range of 120°~140°.
Surgical technique
Position: The patient lies supine on an X-ray transparent operating table, and other things such as a cushion or shelf are placed under the affected limb to help maintain the position. Placing the pad under the ipsilateral hip rotates the affected limb inward without excessive external rotation.
Approach
In most cases, small incisions are made in the tibia, calcaneus, and first metatarsal to place external fixation pins.··
Fibula fractures are more easily fixed from the palpable lateral subcutaneous border.
Fractures of the tibial vault involving the joint can be fixed percutaneously. If soft tissue conditions permit, and if necessary, a regular anterolateral or medial approach can be used for fixation. If external fixation is only used as a temporary fixation measure, the needle entry point where the external fixation needle is planned to be placed should be far away from the final nail fixation area to prevent soft tissue contamination. Early fixation of the fibula and intra-articular fragments facilitates subsequent definitive fixation.
Precautions
Be wary of the external fixation pin track for subsequent definitive fixation of the surgical field, as contaminated tissue will inevitably lead to postoperative complications. Regular anterolateral or medial approaches with significant soft tissue swelling can also lead to serious complications in wound healing.
Reduction and fixation of fibula fractures:
Whenever soft tissue conditions permit, fibula fractures are treated first. The fibular fracture is reduced and fixed using the lateral fibular incision, usually with 3.5mm lag screws and 3.5mm l/3 tube plate, or 3.5mm LCDC plate and screws. After the fibula is anatomically reduced and fixed, it can be used as a standard for restoring the length of the tibia and correcting the rotational deformity of the tibial fracture.
Precautions
Significant soft tissue swelling or a severe open wound may also prevent primary fixation of the fibula. Be careful not to fix proximal fibular fractures and be careful to injure the proximal superficial peroneal nerve.
Tibial Fractures: Reduction and Internal Fixation
Intra-articular fractures of the tibial vault should be reduced under direct vision through the anterolateral or medial approach of the distal tibia, or through indirect manual reduction under fluoroscopy.
When driving the lag screw, the fracture fragment should be fixed with Kirschner wire first.
Early reduction and fixation of intra-articular fractures allows for minimally invasive techniques and greater flexibility in secondary definitive fixation. Unfavorable soft-tissue conditions such as marked swelling or severe soft-tissue damage may prevent early fixation of intra-articular fragments.
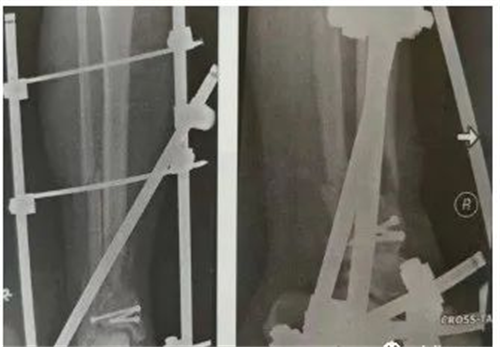
Tibial Fractures: Transarticular External Fixation
A cross-joint external fixator can be used.

According to the requirements of the second-stage definitive fixation method, two 5mm half-threaded external fixation pins were inserted percutaneously or through small incisions on the medial or anterolateral surface of the tibia at the proximal end of the fracture.
First bluntly dissect to the bone surface, then protect the surrounding tissue with a soft tissue protection sleeve, and then drill, tap, and drive the screw through the sleeve.
The external fixation pins at the distal end of the fracture can be placed on the distal tibial fragment, the calcaneus and first metatarsal, or the neck of the talus.
Transcalcaneal external fixation pins should be placed at the calcaneal tuberosity from medial to lateral to prevent damage to the medial neurovascular structures.
The external fixation pin of the first metatarsal should be placed on the anteromedial surface of the base of the first metatarsal.
Sometimes an external fixation pin can be placed anterolaterally through the tarsal sinus incision.
Then, the distal tibia was reset and the force line was adjusted through intraoperative fluoroscopy, and the external fixator was assembled.
When adjusting the external fixator, loosen the connecting clip, perform longitudinal traction, and perform gentle manual reduction under fluoroscopy to adjust the position of the fracture fragment. The operator then maintains the position while the assistant tightens the connecting clips.
Main point
If external fixation is not a definite treatment, the external fixation needle track should be kept away from the definite fixation area during operation planning, so as not to pollute the future operation field. The stability of external fixation can be increased by increasing the spacing of the fixation pins at each fracture site, increasing the diameter of the pins, increasing the number of fixation pins and connecting struts, adding fixation points across the ankle joint, and increasing the fixation plane or applying a ring external fixator . Adequate corrective alignment should be ensured through the anterior-posterior and lateral phases.
Tibial fractures: non-span-articular external fixation
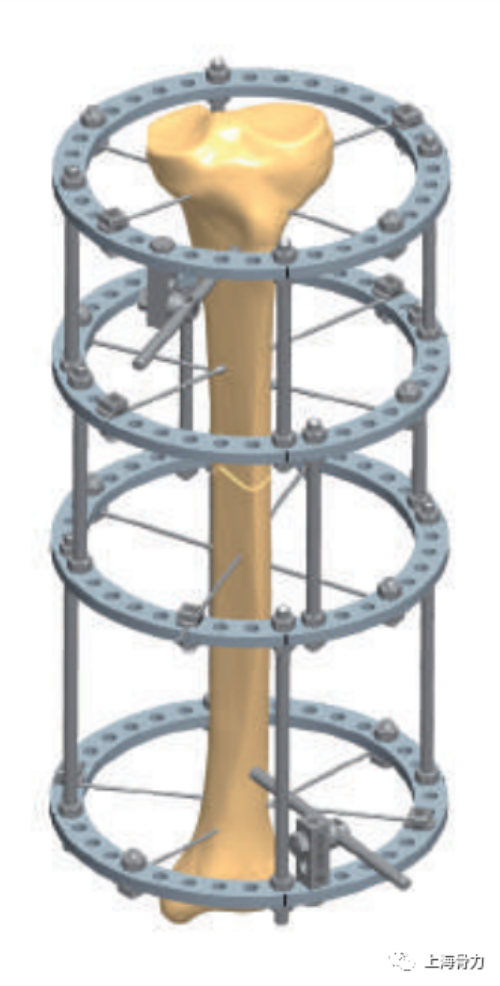
Sometimes it is an option to apply an external fixator that does not span the joint. If the distal tibial fragment is large enough to accommodate half-thread external fixation pins, a simple external fixator can be used. For patients with small metaphyseal fracture fragments, a hybrid external fixator consisting of a proximal semi-threaded external fixation pin and a distal fine Kirschner wire is useful as a temporary or definitive treatment technique . Caution should be exercised when using non-span-articular external fixators for fractures with soft tissue contamination. Removal of this contaminated tissue, debridement of the needle tract, and immobilization of the extremity in a cast until good wound healing is usually necessary before definitive immobilization can be performed.
Sichuan ChenAnHui Technology Co., Ltd
Contact: Yoyo
WhatsApp:+8615682071283
Email: liuyaoyao@medtechcah.com
Post time: Feb-10-2023





