




· Applied Anatomy
In front of the scapula is the subscapular fossa, where the subscapularis muscle starts. Behind is the outward and slightly upward traveling scapular ridge, which is divided into supraspinatus fossa and infraspinatus fossa, for the attachment of supraspinatus and infraspinatus muscles respectively. The outer end of the scapular ridge is the acromion, which forms the acromioclavicular joint with the acromion end of the clavicle by means of a long ovoid articular surface. The superior margin of the scapular ridge has a small U-shaped notch, which is crossed by a short but tough transverse suprascapular ligament, under which the suprascapular nerve passes, and over which the suprascapular artery passes. The lateral margin (axillary margin) of the scapular ridge is the thickest and moves outward to the root of the scapular neck, where it forms a glenoid notch with the edge of the glenoid of the shoulder joint.
· Indications
1. Resection of benign scapular tumors.
2. Local excision of malignant tumor of scapula.
3. High scapula and other deformities.
4. Removal of dead bone in scapular osteomyelitis.
5. Suprascapular nerve entrapment syndrome.
· Body position
Semi-prone position, tilted at 30° to the bed. The affected upper limb is wrapped with a sterile towel so that it can be moved at any time during the operation.
· Operating steps
1. A transverse incision is generally made along the scapular ridge in the supraspinatus fossa and the upper part of the infraspinatus fossa, and a longitudinal incision can be made along the medial edge of the scapula or the medial side of the subscapularis fossa. The transverse and longitudinal incisions can be combined to form an L-shape, inverted L-shape, or a first-class shape, depending on the need for visualization of the different parts of the scapula. If only the upper and lower corners of the scapula need to be exposed, small incisions can be made in the corresponding areas (Figure 7-1-5(1)).
2. Incise the superficial and deep fascia. The muscles attached to the scapular ridge and medial border are incised transversely or longitudinally in the direction of the incision (Fig. 7-1-5(2)). If the supraspinatus fossa is to be exposed, the fibers of the middle trapezius muscle are incised first. The periosteum is incised against the bony surface of the scapular gonad, with a thin layer of fat between the two, and all of the supraspinatus fossa is exposed by subperiosteal dissection of the supraspinatus muscle, along with the overlying trapezius muscle. When incising the upper fibers of the trapezius muscle, care should be taken not to damage the parasympathetic nerve.
3. When the suprascapular nerve is to be revealed, only the fibers of the upper middle part of the trapezius muscle can be pulled upward, and the supraspinatus muscle can be gently pulled downward without stripping, and the white shiny structure seen is the suprascapular transverse ligament. Once the suprascapular vessels and nerves have been identified and protected, the suprascapular transverse ligament can be severed, and the scapular notch can be explored for any abnormal structures, and the suprascapular nerve can then be released. Finally, the stripped trapezius muscle is sutured back together so that it is attached to the scapula.
4. If the upper part of the infraspinatus fossa is to be exposed, the lower and middle fibers of the trapezius muscle and the deltoid muscle can be incised at the beginning of the scapular ridge and retracted upward and downward (Fig. 7-1-5(3)), and after the infraspinatus muscle has been exposed, it can be subperiosteally peeled (Fig. 7-1-5(4)). When approaching the superior end of the axillary margin of the scapular gonad (i.e., below the glenoid), attention should be paid to the axillary nerve and posterior rotator humeral artery passing through the quadrilateral foramen surrounded by the teres minor, teres major, long head of the triceps, and surgical neck of the humerus, as well as the rotator scapulae artery passing through the triangular foramen surrounded by the first three, so as not to cause injury to them (Fig. 7-1-5(5)).
5. To expose the medial border of the scapula, after incising the fibers of the trapezius muscle, the trapezius and supraspinatus muscles are retracted superiorly and externally by subperiosteal stripping to expose the medial portion of the supraspinatus fossa and the upper portion of the medial border; and the trapezius and infraspinatus muscles, together with the vastus lateralis muscle attached to the inferior angle of the scapula, are subperiosteally stripped to expose the medial portion of the infraspinatus fossa, the inferior angle of the scapula, and the lower portion of the medial border.
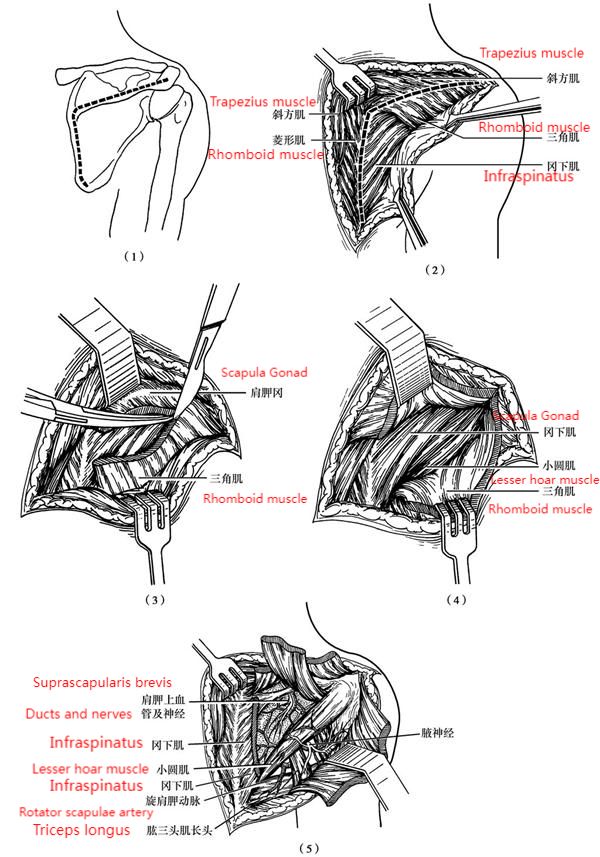
Figure 7-1-5 Path of dorsal scapular exposure
(1) incision; (2) incision of the muscle line; (3) severing the deltoid muscle from the scapular ridge; (4) lifting the deltoid muscle to reveal the infraspinatus and teres minor; (5) stripping the infraspinatus muscle to reveal the dorsal aspect of the scapula with vascular anastomosis
6. If the subscapular fossa is to be exposed, the muscles attached to the inner layer of the medial border, i.e., scapularis, rhomboids and serratus anterior, should be peeled off at the same time, and the whole scapula can be lifted outward. When freeing the medial border, care should be taken to protect the descending branch of the transverse carotid artery and the dorsal scapular nerve. The descending branch of the transverse carotid artery originates from the thyroid neck trunk and travels from the upper angle of the scapula to the lower angle of the scapula via the scapularis tenuissimus, rhomboid muscle and rhomboid muscle, and the rotator scapulae artery forms a rich vascular network in the dorsal part of the scapula, so it should be tightly adhered to the surface of the bone for the subperiosteal peeling.
Post time: Nov-21-2023





