




- Indications
1).Severe comminuted fractures have obvious displacement, and the articular surface of the distal radius is destroyed.
2).The manual reduction failed or the external fixation failed to maintain the reduction.
3).Old fractures.
4).Fracture malunion or nonunion. bone present at home and abroad
- Contraindications
Elderly patients who are not suitable for surgery.
- Internal fixation (volar approach)
Routine preoperative preparation. Anesthesia is performed using brachial plexus anesthesia or general anesthesia
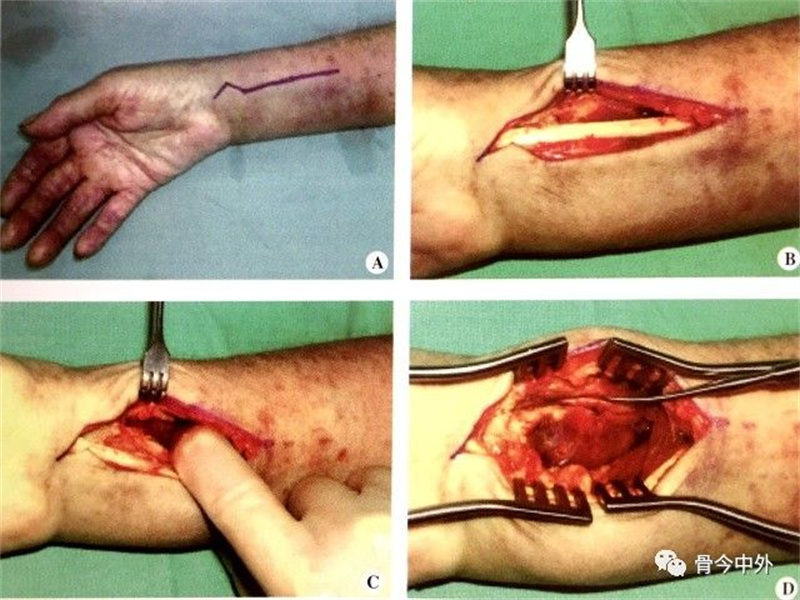
1).The patient is placed in a supine position with the affected limb abducted and placed on the surgical frame. An 8cm incision is made between the radial artery of the forearm and the flexor carpi radialis muscle and extended to the wrist crease. This can completely expose the fracture and prevent scar contracture. The incision does not need to go into the palm of the hand (Figure 1-36A).
2).Follow the incision to the flexor carpi radialis tendon sheath (Figure 1-36B), open the tendon sheath, incise the deep anterior bamboo fascia to expose the flexor pollicis longus, use the index finger to project the flexor pollicis longus to the ulnar side, and partially free the flexor pollicis longus. The muscle belly is fully exposed to the pronator quadratus muscle (Figure 1-36C)
3).Make an “L” shaped incision along the radial side of the radius to the radial styloid process to expose the pronator quadratus muscle, and then peel it off from the radius with a peeler to expose the entire bamboo fold line (Figure 1-36D, Figure 1-36E)
4).Insert a stripper or a small bone knife from the fracture line, and use it as a lever to reduce the fracture. Insert a dissector or a small scissor knife across the fracture line to the lateral bone cortex to relieve compression and reduce the distal fracture fragment, and use fingers to compress the dorsal fracture fragment to reduce the dorsal fracture fragment.
When the radial styloid fracture is fractured, it is difficult to reduce the radial styloid fracture due to the pull of the brachioradialis muscle. To reduce the force of the pull, the brachioradialis can be manipulated or dissected from the distal radius. If necessary, the distal fragment can be temporarily fixed to the proximal fragment with Kirschner wires.
If the ulnar styloid process is fractured and displaced, and the distal radioulnar joint is unstable, one or two Kirschner wires can be used for percutaneous fixation, and the ulnar styloid process can be reset by the volar approach. Smaller fractures usually do not require manual treatment. However, if the distal radioulnar joint is unstable after fixation of the radius, the styloid fragment can be excised and the edges of the triangular fibrocartilage complex sutured to the ulnar styloid process with anchors or silk threads.
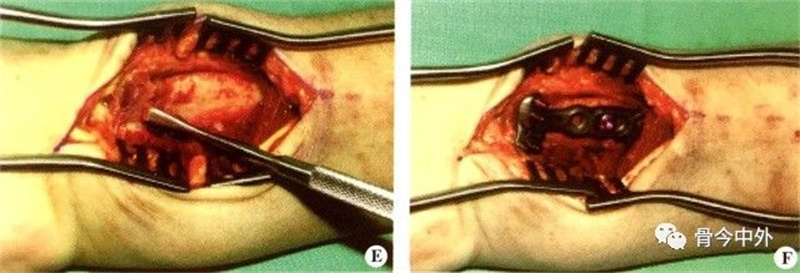
5).With the help of traction, the joint capsule and ligament can be used to release the intercalation and reduce the fracture. After the fracture is successfully reduced, determine the placement position of the volar steel plate under the guidance of X-ray fluoroscopy and screw a screw into the oval hole or sliding hole to facilitate position adjustment (Figure 1-36F). Use a 2.5mm drill hole to drill the center of the oval hole, and insert a 3.5mm self-tapping screw.
Figure 1-36 Skin incision (A); incision of the flexor carpi radialis tendon sheath (B); peeling off part of the flexor tendon to expose the pronator quadratus muscle (C); splitting the pronator quadratus muscle to expose the radius (D); exposing the fracture line (E); place the volar plate and screw in the first screw (F)
6).Use C-arm fluoroscopy to confirm proper plate placement. If necessary, push the plate distally or proximally to obtain the best distal screw placement.
7).Use a 2.0mm drill to drill a hole at the far end of the steel plate, measure the depth and screw in the locking screw. The nail should be 2mm shorter than the measured distance to prevent the screw from penetrating and protruding from the dorsal cortex. Generally, a 20-22mm screw is sufficient, and the one fixed on the radial styloid process should be shorter. After screwing in the distal screw, screw it Insert the remaining proximal screw.
Because the angle of the screw is designed, if the plate is placed too close to the distal end, the screw will enter the wrist joint. Take tangential slices of the articular subchondral bone from the coronal and sagittal positions to evaluate whether it enters the joint, and then follow the instructions Adjust the steel plates and/or screws

(Figure1-37) Figure 1-37 Fixation of distal radius fracture with volar bone plate A. Anteroposterior and lateral X-ray film of distal radius fracture before operation, showing the displacement of the distal end to the volar side; B. Anteroposterior and lateral X-ray film of postoperative fracture, showing fracture Good reduction and good wrist joint clearance
8).Suture the pronator quadratus muscle with non-absorbable sutures. Note that the muscle will not completely cover the plate. The distal part should be covered to minimize the contact between the flexor tendon and the plate. This can be achieved by suturing the pronator quadratus to the edge of the brachioradialis, closing the incision layer by layer, and fixing it with plaster if necessary.
Post time: Sep-01-2023





