




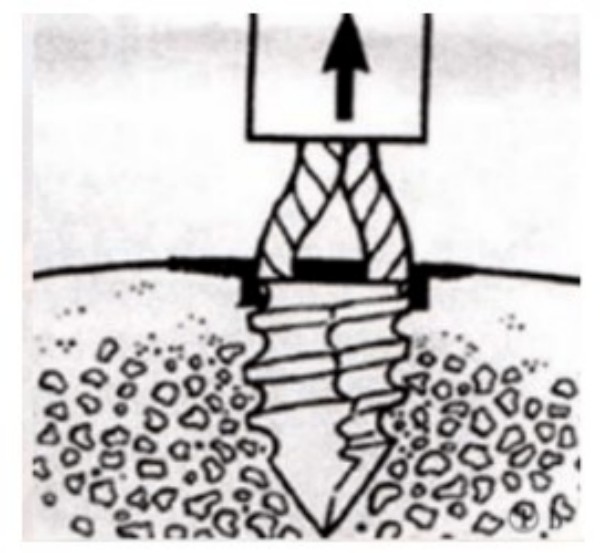
In the early 1990s, foreign scholars took the lead in using suture anchors to repair structures such as the rotator cuff under arthroscopy. The theory originated from the underground “sinking object” support principle in South Texas, USA, that is, by pulling the underground steel wire at a 45° sinking angle to the ground, the underground building is firmly fixed on the “sinking object” at the other end of the steel wire.
Sports medicine originated from orthopedic traumatology. It is a basic and clinical multidisciplinary comprehensive application of medicine and sports. The goal is to achieve maximum functional repair with minimal trauma, including meniscus injury, cruciate ligament injury, rotator cuff tear, shoulder dislocation instability, SLAP injury, etc. are all within the scope of sports medicine treatment
Anchor is a medical device commonly used in sports medicine and orthopedic surgery. It is mainly used to fix soft tissues (such as tendons, ligaments, etc.) to bones to promote tissue healing and recovery. Anchors are usually made of biocompatible materials to ensure safety and stability in the body.


According to the material classification of anchors, there are two main categories: non-biodegradable anchors and biodegradable anchors.
The main materials of non-biodegradable anchors are titanium, nickel-titanium alloy, stainless steel, titanium and poly-L-lactic acid; most of the suture anchors used in clinical practice are made of metal materials, which have the advantages of good holding force, easy implantation and easy X-ray evaluation.
The main materials of biodegradable anchors are poly-D-lactic acid, poly-L-lactic acid, polyglycolic acid, etc. Compared with non-biodegradable anchors, biodegradable anchors are easy to revise, have little interference with images, and are absorbable. They can also be used for children.
Main materials of anchors
1. Metal anchors
• Materials: Mainly metal materials such as titanium alloy.
• Features: Strong and durable, able to provide stable fixation effect. However, imaging artifacts may occur and there is a risk of falling off.
2. Absorbable anchors
• Materials: absorbable materials such as polylactic acid (PLLA).
• Features: Gradually degraded in the body, no secondary surgery is required for removal. However, the degradation rate may be unstable, and the fixation strength may decrease over time.
3. Polyetheretherketone (PEEK) anchors
• Materials: high-performance polymers such as polyetheretherketone.
• Features: Provides higher nail body strength and mechanical properties, while having good biocompatibility and ideal postoperative imaging effects.
4. All-suture anchors
• Composition: Mainly composed of inserter, anchor and suture.
• Features: Very small in size, soft in texture, suitable for situations where native bone mass is lost or the implant site is limited.

According to the design characteristics of anchors, they can be divided into two categories: knotted anchors and knotless (such as full suture) anchors:
1. Knotted anchors
Knotted anchors are traditional anchor types, characterized by a section of suture connected to the tail of the anchor. The doctor needs to pass the suture through the soft tissue with a needle and tie a knot to fix the soft tissue to the anchor, that is, the bone surface.
• Material: Knotted anchors are usually made of non-absorbable materials (such as titanium alloy) or absorbable materials (such as polylactic acid).
• Mechanism of action: The anchor is fixed in the bone through threads or expansion wings, while the suture is used to connect the soft tissue to the anchor, and a stable fixation effect is formed after tying the knot.
• Advantages and disadvantages: The advantage of knotted anchors is that the fixation effect is reliable and suitable for a variety of soft tissue injuries. However, the knotting process may increase the complexity and time of the operation, and the presence of the knot may lead to local tension concentration, increasing the risk of suture breakage or anchor loosening.
2. Knotless anchors
Knotless anchors, especially full suture anchors, are a new type of anchor developed in recent years. Its characteristic is that the entire anchor is composed of sutures, and soft tissue fixation can be achieved without tying knots.



• Materials: Full suture anchors usually use soft and strong suture materials, such as ultra-high molecular weight polyethylene (UHMWPE) fibers.
• Mechanism of action: Full suture anchors can be directly embedded in bone tissue through their special suture structure and implantation method, while using the tension of the suture to tightly fix the soft tissue to the bone surface. Since there is no need to tie knots, the complexity and time of the operation are reduced, and the risk of suture breakage and anchor loosening is also reduced.
• Advantages and disadvantages: The advantages of full suture anchors are simple surgical operation, reliable fixation effect and little damage to soft tissue. However, due to its special structure, it has high requirements for surgical techniques and implantation location. In addition, the price of full suture anchors may be relatively high, which increases the financial burden on patients.
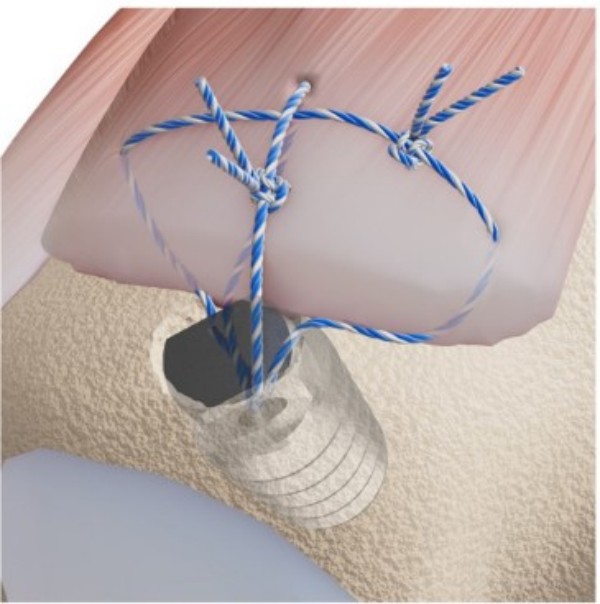
Anchors are widely used in various sports medicine surgeries, such as rotator cuff repair, tendon fixation, ligament reconstruction, etc. The following is an introduction to the surgical application of anchors using rotator cuff repair as an example:
• Surgical steps: First, the doctor will clean and prepare the rotator cuff injury site; then, implant the anchor in the appropriate position; then, use sutures to fix the rotator cuff tissue to the anchor; finally, suture and bandage.
• Surgical effect: Through the fixation of the anchor, the stability and function of the rotator cuff tissue can be restored, promoting the patient’s recovery.
Advantages, Disadvantages and Precautions of Anchors
Advantages
• Provides stable fixation.
• Applicable to a variety of soft tissue injuries.
• Some anchors are absorbable and do not require secondary surgery for removal.
Disadvantages
• Metal anchors may produce imaging artifacts.
• The degradation rate of absorbable anchors may be unstable.
• There is a risk of anchor detachment or suture breakage.
Sports medicine anchors can be used for the following surgeries:
1. Recurrent lateral epicondylitis (tennis elbow) that has not been effectively treated for multiple times: When conservative treatment is ineffective, surgical treatment can be chosen, and the anchor can be used to reconnect the insertion point of the radial extensor carpi brevis to the lateral epicondyle of the humerus.
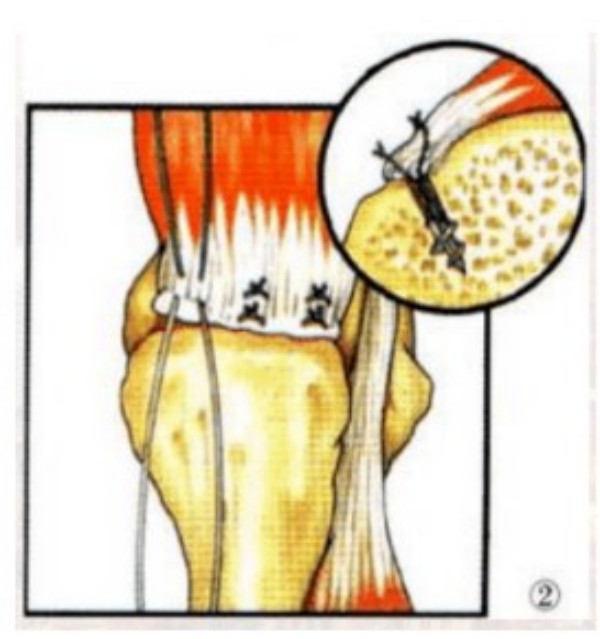
2. Distal biceps tendon tear: Tears caused by abnormal range of motion, traction, impact, etc. can be treated with wire anchors. Two anchors are buried in the radial tuberosity, and the tail wire is sutured to the biceps tendon stump.
3. Elbow collateral ligament rupture: Posterior dislocation of the elbow is often accompanied by ulnar collateral ligament injury, especially anterior bundle injury. For elbow collateral ligament injury, more scholars tend to prefer early surgical treatment. The wire anchor method is used to roughen the bone surface where the ligament is attached. After fresh bleeding, the anchor is screwed into the bone surface where the ligament is attached, and the braided wire at the end of the nail is used to braid the ligament stump and tighten it or repair the ligament with a needle.
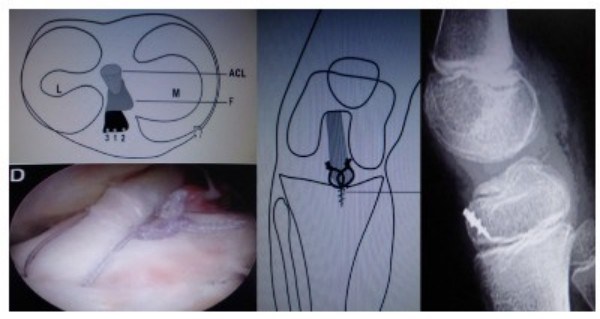
4. Fracture of the inferior attachment point of the cruciate ligament: Anterior cruciate ligament (ACL) tibial attachment point avulsion fracture is a special type of ACL injury and should be repaired early. The use of wire anchor method has a wide range of indications and is not limited by the size of the fracture fragment. It does not require intraoperative fluoroscopy to adjust the direction of the screw. The operation is relatively simple and the operation time is correspondingly shortened.
5.Patellar instability: caused by bony anatomical abnormalities and insufficient soft tissue restriction. Most scholars advocate active surgical treatment using wire anchors.

6. Patellar inferior pole fracture: The wire anchor technology can be used to treat patellar inferior pole fracture. By fixing the patellar inferior pole fracture and weaving and suturing the patellar ligament, the integrity of the knee extensor mechanism can be restored and the effective physiological length of the knee extensor mechanism can be maintained.
7. Suitable for the connection and fixation of bones and soft tissues in knee, spinal cord, shoulder, elbow, ankle, foot, wrist and hand surgeries: The anchor has a corrugated thread design, which is easy to implant and provides stronger pull-out resistance, and is suitable for surgeries in various parts.
Precautions
• The patient’s bone condition and the anatomical structure of the surgical site should be fully evaluated before surgery.
• Select the appropriate anchor type and specifications to ensure the surgical effect.
• Appropriate rehabilitation exercises should be performed after surgery to promote tissue healing and restore function.
In summary, anchors play an important role in sports medicine. By selecting the appropriate anchor type and specifications and following the correct surgical steps and precautions, the surgical effect can be ensured and the patient’s recovery can be promoted.
Post time: Dec-17-2024





